Download
1 / 45
450 likes | 953 Views
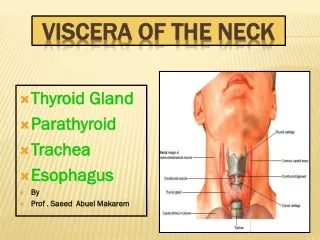
Primary Tumors of the Neck. Carotid Body Tumor. Rare tumor Higher incidence in areas where people live at high altitudes because of chronic hypoxia leading to carotid body hyperplasia Asscociated with phaeochromocytoma

E N D
Carotid Body Tumor • Rare tumor • Higher incidence in areas where people live at high altitudes because of chronic hypoxia leading to carotid body hyperplasia • Asscociated with phaeochromocytoma • Also known as Chemodectomaas they arise from chemoreceptor cells on the medial side of the carotid bulb
Carotid body tumours are derived from both, the mesoderm of the second branchial arch and the ectoderm of the neural crest. • Also called paragangliomasbecause they arise from the paraganglionic cells • Malignant potential in 2.6 - 5% of the cases. • Lymphatics are the most favoured route of spread
CLINICAL FEATURES • Long duration, usually unilateral • Slow enlarging painless lump at the carotid bifurcation • Mass is firm, rubbery • Pulsatile(transmitted pulsation) • Mobile from side to side but not up & down • 1/3rd of the patients present with pharyngeal mass that pushes the tonsils medially & anteriorly • Thrill & bruit may be ellicited
INVESTIGATIONS • Carotid Angiogram is the investigation of choice • It usually demonstrates the splaying of the carotid bifurcation & a blush which outlines the tumor cells • MRI • TUMOR MUST NOT BE BIOPSIED & FNAC IS ALSO CONTRAINDICATED
DIFFERENTIAL DIAGNOSIS • Vagal body tumor (Neurofibroma of the Vagus) • Carotid artery aneurysm • Sarcoma • Lymph nodes
TREATMENT • As the tumors rarely metastasize & their overall rate of growth is slow surgery is not usually indicated • When indicated & tumor is small it may be possible to dissect the tumor away from the carotid bifurcation • Large tumors require resection. • They do not respond to radiotherapy
VAGAL BODY TUMORS • Vagalparagangliomas arise from nests of paraganglionic tissue of the vagus nerve just below the base of the skull near the jugular foramen • May also be found at various site along the nerve down to the level of carotid artery bifurcation
CLINICAL FEATURES Long history of 2 to 3 yrs Slow growing Painless masses in the anterolateral aspect of neck They may spread into the cranial cavity
DIAGNOSIS 1)MRI 2) CT 3) Arteriography TREATMENT Surgical excision
PERIPHERAL NERVE TUMORS • NEUROFIBROMA It is a benign tumor arising from the connective tissue of the nerve containing ectodermal neural & mesodermal connective tissues It can be single or multiple SITES • Cranial • Spinal • Peripheral
TYPES A) Nodular Neurofibroma • Single, smooth, firm, tender • Moves perpendicular to the direction of the nerve • Presents with pain & hyperaesthesia in the distribution of the nerve
B) PLEXIFORM NEUROFIBROMA Occurs along the distribution of 5th cranial nerve in the skin of face Occurs in the cutaneous distribution of the peripheral nerve attains enormous size causes bone erosion, orbit & deeper structure May also cause myxomatous degeneration Parasthersia along the distribution of the trigeminal nerve(ophthalmic division)
C) VON RECKLINGHAUSEN’s DISEASE • Inherited autosomal dominant disease involving chromosome 17 • Maybe cranial, spinal or peripheral • Café au lait spots- coffee colored, usually 5 in number, 1.5 cm or more in size signifying common neuroectodermal origin of nerve sheath cells & melanocytes • Lisch nodules • Associated with MEN IIb
COMPLICATIONS • Sarcomatous change • Cystic degeneration • Haemorrhage • Neurological defects • Erosion of bone • Muscle atrophy TREATMENT Exicision
NEURILEMMOMA • Also called Schwannoma • Ectodermal in origin, arising from the neurilemmal cells • Lobulated, encapsulated, soft, whitish grey • Commonly seen in the acoustic nerve TYPES • Anthony A- 2 rows of spindle cells with central acellular area • Anthony B – Acellularmyloid areas
Metastatic spread from squamous carcinoma to the cervical lymph nodes is a common occurrence from head & neck primary cancers • Common sites of primary • Nasopharynx • Tonsil • Tongue • Pyriformfossa • Supraglottic larynx
Classification • Level 1: Submental (Ia) Submandibular (Ib). • Level 2: Upper deep cervical region. • Level 3: Middle cervical region. • Level 4: Internal jugular below omohyoid. • Level 5: Posterior triangle. (also known as accessory chain) • Level 6: Adjacent to thyroid. • Level 7: Tracheal esophageal groove and superior mediastinum.
Features • Usually painless, rapidly growing • Hard in consistency, nodular surface, fixed • Secondaries can infiltrate into carotids, sternomastoid, posterior vertebral muscles, spinal accessory nerve, hypoglossal nerve,cervical sympathetic chain • They can also cause ulceration & fungation of skin • Dysphagia, dyspnoea, haemoptysis, hoarseness of voice, ear pain, deafness, torrential haemorrhage may result depending on the site of primary
TYPES 1)SECONDARIES IN THE NECK WITH KNOWN PRIMARY • Here secondaries are present along with a known primary • Usaually biopsy from the primary & FNAC from the secondary are done • Primary is treated either by surgery or by curative radiotherapy • Secondaries when mobile are treated by radical lymph node block dissection in the neck
SECONDARIES IN THE NECK WITH CLINICALLY UNIDENTIFIED PRIMARY • Hard, neck nodes are secondaries but primary not identified Investigations • nasopharyngoscopy • Laryngoscopy • Oesophagoscopy • Bronchoscopy • Biopsies from fossa of rosenmuller. Lateral wall of pharynx • FNAC of thyroid • CT scan Once the biopsy confirms the primary, it is treated either by surgery or by curative radiotherapy Secondaries in the neck are treated by radical neck dissection
Here secondaries in the neck lymph nodes are confirmed by FNAC but primary has not been revealed clinically & by any available investigations • SECONDARIES IN THE NECK WITH OCCULT PRIMARY • Fossa of Rosenmuller • Lateral wall of the pharynx • Posterior third of the tongue • Thyroid • Paranasal sinuses • Bronchus • oesophagus
In upper & mid cervical region 80% are due to squamous cell carcinomas • In lower cervical and supraclavicular region 40% can be adenocarcinomas REASONS FOR BEING OCCULT • Too small a primary to detect • Possibility of immunological spontaneous regression • Inability of diagnostic tools to detect the primary
TREATMENT • Initially secondaries in the neck are treated by radical neck dissection • Regular follow ups are done at 3 month intervals until the primary is revealed • Once primary is revealed, it is confirmed by biopsy & treated accordingly either by curative radiotherapy or wide exicision
Clinical Nodal Staging • NX: Not assessable. • N0: No clinically positive nodes. • N1: Single clinically positive ipsilateral node less than or equal to 3 cm • N2: Greater than 3 cm, less than 6 cm • N2A: Single, ipsilateral. • N2B: Multiple ipsilateral. • N3: Greater than 6 cm • N3A: Ipsilateral. • N3B: Bilateral. • N3C: Contralateral
INVESTIGATIONS • FNAC of the secondary • Biopsy from the primary • Nasopharyngoscopy, laryngoscopy, bronchoscopy, oesophagoscopy • CT scan • Chest X-ray • MRI/ PET scan • Triple endoscopy (direct/indirect laryngoscopy,oesophagoscopy & bronchoscopy)
DIFFERENTIAL DIAGNOSIS • Lymphomas • Tuberculous lymphadenitis • Non-specific lymphadenitis • HIV • Chronic lymphatic leukemia
TYPES OF NECK DISSECTION 1) Radical neck dissection; 2) Modified radical neck dissection; 3) Selective neck dissection supraomohyoid, posterolateral, Lateral anterior 4) Extended radical neck dissection.
RADICAL NECK DISSECTION • It defined as removing all of the lymphatic tissue in regions I-V including removal of the spinal accessory nerve(SAN), sternocleidomastoid muscle (SCM) internal jugular vein (IJV).
INDICATIONS • in patients with • extensive cervical lymph node metastasis and/or extension beyond the capsule with invasion into the spinal accessory nerve, IJV, and SCM. • Many surgeons will elect to perform a RND if there is extensive disease surrounding the spinal accessory nerve without gross evidence of invasion.
MODIFIED RADICAL NECK DISSECTION is defined as excision of all lymph nodes routinely removed by radical neck dissection with preservation of one or more nonlymphatic structures, i.e.,SAN, IJV, SCM. 4 Medina subclassifies the MRND into types I-III; • typeI preserves the SAN, • typeII preserves the SAN and IJV, • typeIII preserves the SAN, IJV,&SCM. type III referred to as the "functional neck dissection" (Bocca), *in his classic description the submandibular gland is not excised.
Indications • in patients with gross nodal metastasis to the neck that does not directly infiltrate or adhere to the non-lymphatic structures • Bilateral MRND is indicated when there is contralateral nodal involvement
Selective neck dissection • is defined as any type of cervical lymphadenectomy where there is preservation of one or more lymph node groups removed by the radical neck dissection. • There are four common subtypes,
SUPRAOMOHYOID NECK DISSECTION • This removes lymph tissue contained in regions I-III.
Indications • patients with primary tumors arising from the oral cavity without clinical or radiologic evidence of cervical metastasis but who have a high probability of occult lymphatic disease. • in patients with staged T2-T4N0 or TXN1 when the palpable node is less than 3 cm, clearly mobile, and located in levels I or II. • Bilateral SOHND is indicated in patients who have carcinomas of the anterior tongue or oral tongue and floor of mouth.
Posterolateral neck dissection, refers to the removal of the suboccipital lymph nodes, retroauricular lymph nodes, levels II-IV, and level V Medina suggests subclassification of the posteriolateral neck dissection to types I-III to mirror preservation of SAN, IJV, and SCM as in MRND.
Indications • This type of neck dissection is primarily used to treat the neck in patients with cutaneous malignancies and soft tissue sarcomas.
Lateral neck dissection removes lymph tissue in levels II-IV. Indications removal of nodal disease associated with carcinomas arising in the oropharynx, hypopharynx, and larynx.
Anterior neck dissection • is the last subtype of selective neck dissection and refers to the removal of lymph nodes surrounding the visceral structures of the anterior aspect of the neck
Indications • (1) selected cases of differentiated thyroid carcinoma, • (2) parathyroid carcinoma • (3) subglottic carcinoma • (4) glottic carcinomas with subglottic extension,
Extended neck dissection • defined as removal of one or more additional lymph node groups and/or nonlymphatic structures not encompassed by radical neck dissection, such as parapharyngeal, superior mediastinal, and paratracheal.
Indications • Extended neck dissections are usually performed when MRND or RND is planned for N+ necks. • The decision to extend the neck dissection may either be made preoperatively based on findings on CT or MRI or intraoperatively based on findings of tumor invasion of surrounding structures. • The most significant example is when cervical disease involves the carotid artery.
Radiotherapy Along with RND when : • lymph node more than 3 cm • multiple • extra capsular invasion. • occult primary