Download
1 / 31
310 likes | 533 Views
Prevention of Venous Thromboembolism in Patients With Cancer. Supplement to Module 5. Outline. Introduction Thromboprophylactic modalities Thromboprophylaxis in medical cancer patients Thromboprophylaxis in cancer surgery Thromboprophylaxis in patients with central venous catheters.

E N D
Prevention of Venous Thromboembolism in Patients With Cancer Supplement to Module 5
Outline • Introduction • Thromboprophylactic modalities • Thromboprophylaxis in medical cancer patients • Thromboprophylaxis in cancer surgery • Thromboprophylaxis in patients with central venous catheters
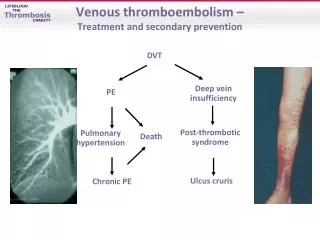
Introduction • Cancer is a key risk factor for VTE • Associated with an approximately 6-fold increased risk for thromboembolic complications1, 2 • Number 2 cause of death in cancer patients3 • VTE also has serious long-term implications for the cancer patient4 • High recurrence rates • High risk for hemorrhagic complications in patients treated with anticoagulants • Identification of at-risk patients and thromboprophylaxis is critical • A careful balance must be struck between adequate thromboprophylaxis and bleeding risk 1. Heit JA et al. Arch Intern Med. 2000;160:809-815. 2. Blom JW et al. JAMA. 2005;293:715-722. 3. Rickles FR, Edwards RL. Blood. 1983;62:14-31. 4. Prandoni P et al. Blood. 2002;100:3484-3488.
Outline • Introduction • Thromboprophylactic modalities • Thromboprophylaxis in medical cancer patients • Thromboprophylaxis in cancer surgery • Thromboprophylaxis in patients with central venous catheters
Mechanical Thromboprophylaxis • Several mechanical modalities are available • Aggressive, early mobilization • Electrical calf stimulation • Intermittent pneumatic compression • Graduated static compression stockings • Venous foot pump devices • All devices are intended to increase venous outflow and/or reduce stasis within the leg veins
Advantages Do not increase the risk of bleeding Can be used in patients at high bleeding risk Efficacy has been demonstrated in a number of patient groups May enhance the effectiveness of anticoagulant thromboprophylaxis May reduce leg swelling Selected Limitations Not as intensively studied as pharmacologic thromboprophylaxis No established standards for use In high-risk groups, mechanical modalities are less effective than anticoagulant thromboprophylaxis Greater effect in reducing calf DVT than proximal DVT Effect on PE and death unknown Compliance by patients and staff often poor Cost: associated with purchase, storage, dispensing, and cleaning of the devices, as well as ensuring optimal compliance Advantages and Disadvantages of Mechanical Thromboprophylaxis Geerts WH et al. Chest. 2008;133:381S-453S.
Inferior Vena Caval Filters • Use largely restricted to patients with contraindications or failure of anticoagulant therapy • Study by Decousus (1998) found a 78% reduction in risk for early PE • Early efficacy counterbalanced by a substantial increase in recurrent DVT • At 2 years, 20.8% of patients in filter group and 11.6% of those in the no-filter group had recurrent DVT Decousus H et al. N Engl J Med. 1998;338:409-415.
Pharmacologic Thromboprophylaxis • Multiple modalities are available for pharmacologic thromboprophylaxis • Oral anticoagulants • Unfractionated heparin (UFH) • Low-molecular-weight heparins (LMWH) • Factor Xa inhibitors (fondaparinux) • Profoundly reduce risk for VTE • May be associated with considerable increases in risk for bleeding
Warfarin and Related Oral Anticoagulants • Coumarin derivatives antagonize vitamin K1 • Warfarin is rapidly absorbed and has a long half-life of 36 to 42 h1 • Subject to considerable intra-individual dose-response variation1 • Requires close monitoring to maintain patients within INR target range • In cancer patients, the normal relationship between INR and bleeding or thrombosis is weakened2 • In 1 study, cancer patients with INR 2.0-3.0 had a higher incidence of recurrence (27.1 vs 9.0 per 100 patient-years) and bleeding (13.3 vs 2.1 per 100 patient-years) compared with noncancer patients • Therapeutic INRs are more difficult to achieve and sustain in cancer patients3 1. Zacharski LR et al. Oncologist. 2005;10:72-79. 2. Hutten BA et al. J Clin Oncol. 2000;18:3078-3083. 3. Bona RD et al. Thromb Haemost. 1995;74:1055-1058.
Unfractionated Heparin • Heterogenous mixture of glycosaminoglycans • A unique pentasaccharide produces a conformational change in AT, accelerating inactivation of several anticoagulation enzymes • IV or SC administration in accordance with published dose-adjustment nomograms • Anticoagulant effect monitored by aPTT • Narrow therapeutic window, must be carefully monitored to achieve adequate safety and efficacy Hirsh J et al. Chest. 1998;114:489S-510S.
Low-Molecular-Weight Heparins • Derived from UFH by chemical or enzymatic depolymerization • Results in a fraction with reduced binding affinity for proteins and cells • Relative to heparin: • Reduced inhibitory activity against factor Xa relative to thrombin, • More favorable risk-benefit profile • Superior pharmacokinetic performance Hirsh J et al. Chest. 1998;114:489S-510S.
Low-Molecular-Weight Heparins • Typically administered in fixed or weight-adjusted doses for thromboprophylaxis • Laboratory monitoring generally not necessary • Use of UFH instead of LMWH, or a 50% dose reduction, is recommended in patients with severe renal insufficiency Hirsh J et al. Chest. 1998;114:489S-510S.
Factor Xa Inhibitor (Fondaparinux) • Potentiates neutralization of Factor Xa by antithrombin ~300-fold • Given at a fixed dose of 2.5 mg SC for thromboprophylaxis • Generally not monitored • Dose reductions may be warranted in patients with severe renal insufficiency Hirsh J et al. Chest. 1998;114:489S-510S.
Outline • Introduction • Thromboprophylactic modalities • Thromboprophylaxis in medical cancer patients • Thromboprophylaxis in cancer surgery • Thromboprophylaxis in patients with central venous catheters
Evidence in General Medical Patients • A number of large-scale, well-designed clinical trials have examined thromboprophylaxis in general medical patients • In general, patients with cancer constitute only a small proportion of the patients enrolled in these trials
The MEDENOX Study • Enrolled 1102 acutely ill, hospitalized medical patients (14% with previous or current cancer) • Patients randomized for 6 to 14 days of treatment with: • 20 mg enoxaparin once daily • 40 mg enoxaparin once daily • Placebo once daily • Primary outcome measure: VTE between days 1 and 14 Samama MM. N Engl J Med. 1999;341:793-800.
Enoxaparin Reduced Risk for VTE in Hospitalized, Acutely Ill Patients Samama MM. N Engl J Med. 1999;341:793-800.
The PREVENT Study • Enrolled 3705 acutely ill medical patients (5% with cancer) • Patients randomized for 14 days of treatment with: • Dalteparin 5000 IU SC • Placebo • Primary end point: Incidence of VTE by day 21 Leizorovicz A et al. Circulation. 2004;110:874-879.
Dalteparin Reduced the Incidence of VTE in Acutely Ill Medical Patients • Dalteparin reduced the incidence of VTE from 4.96% in the placebo group to 2.77% in the dalteparin group • Reduction in risk: 45% (P=.0015) • Dalteparin reduced the incidence of symptomatic VTE by 30% • Reductions in risk observed across all major subgroups • Bleeding risk nonsignificantly higher with dalteparin Leizorovicz A et al. Circulation. 2004;110:874-879.
The ARTEMIS Study • Enrolled older, acutely ill medical patients • 15% of patients had cancer • Patients randomized for 6 to 14 days of treatment with: • Fondaparinux 2.5 mg SC • Placebo • Primary outcome measure: DVT and symptomatic VTE on days 6 to 15 Cohen AT et al. BMJ. 2006;332:325-329.
Fondaparinux Reduced Risk for VTE in a Population of Older, Acutely Ill Medical Patients • VTE was observed in 5.6% of fondaparinux patients and 10.5% of placebo patients • 46.7% reduction in relative risk for fondaparinux • Fondaparinux was associated with an improvement in survival that approached statistical significance • Rates of major bleeding were identical in the 2 groups • Minor bleeding was somewhat more frequent in the fondaparinux group (2.6%) than in the placebo group (1.0%) Cohen AT et al. BMJ. 2006;332:325-329.
Studies in Hospitalized Cancer Patients • Levine 19941 • Small study (n=311) of breast cancer patients • Low-dose warfarin vs placebo continued until 1 week after end of chemotherapy • 85% reduction in risk for thromboembolic events • TOPIC-I2 • Certoparin vs placebo in breast cancer patients • No significant difference in rate of VTE or bleeding • TOPIC-II2 • Certoparin vs placebo in NSCLC patients • Risk for VTE reduced from 8.3% to 4.5% with certoparin at 6 months (P=NS) 1. Levine M et al. Lancet. 1994;343:886-889. 2. Haas S. In: Khorana AA and Francis CW, eds: Cancer-associated thrombosis: New findings in translational science. Informa Healthcare. 2008.
Outline • Introduction • Thromboprophylactic modalities • Thromboprophylaxis in medical cancer patients • Thromboprophylaxis in cancer surgery • Thromboprophylaxis in patients with central venous catheters
Heparin as Thromboprophylaxis in Surgical Patients 1. Rem J et al. Schweiz Med Wochenschr. 1975;105:827-835. 2. Gallus AS et a;. JAMA. 1976;235:1980-1982.
LMWH vs UFH: DVT Rates in Cancer Surgical Patients Summary developed by Petralia G et al. In: Khorana AA and Francis CW, eds: Cancer-associated thrombosis: New findings in translational science. Informa Healthcare. 2008.
LMWH Dosage • Increased LMWH dosages may provide incrementally better efficacy in preventing DVT Bergqvist D et al. Br J Surg. 1995;82:496-501.
LMWH Duration • Extended-duration LMWH (4 weeks) provides superior protection to short-term (1 week) therapy Bergqvist D et al. N Engl J Med. 2002;346:975-980.
Fondaparinux in Surgical Patients • 68% of patients in this study underwent surgery for cancer • Fondaparinux and LMWH have similar efficacy and safety in this patient population Agnelli G et al. Br J Surg. 2005;92:1212-1220.
Outline • Introduction • Thromboprophylactic modalities • Thromboprophylaxis in medical cancer patients • Thromboprophylaxis in cancer surgery • Thromboprophylaxis in patients with central venous catheters
Is Thromboprophylaxis Warranted in Patients with CVCs? • Meta-analysis of 15 trials that evaluated UFH, oral fixed low-dose VKAs, LMWHs Kirkpatrick A et al. Am J Med. 2007;120:901 e901-e913.
Is Thromboprophylaxis Warranted in Patients with CVCs? • No statistically significant difference in the risk for catheter-related thrombosis with warfarin, UFH, or LMWH vs placebo Chaukiyal P et al. Thromb Haemost. 2008;99:38-43.