Download
1 / 48
490 likes | 595 Views
Fever without focus. Dr Rafat Mosalli. Question 1.

E N D
Fever without focus Dr Rafat Mosalli
Question 1 • A 3 week old male infant is brought to your ED with a 2 day history of fever. He was born by uncomplicated vaginal delivery at 37 weeks gestation following a normal pregnancy.. His vital signs are: T 38.9C (R), HR 140, RR 40, and BP 90/60. He is sleepy but easily arousable. Physical exam is normal apart from a slightly dull left tympanic membrane. WBC is 16,000, his UA shows 3 WBC/hpf. BC and UC are sent. Your management at this point would consist of: a. Discharge on antipyretics with close follow-up b. Discharge on oral amoxicillin with close follow-up c. LP and admission for parenteral antibiotics d. CXR to r/o pneumonia e. Stool for analysis and culture, and outpatient follow-up
Question 2 • A 7 week old girl is referred in to ED for evaluation of a rectal temperature of 39.2C. Her PE is normal. Her UA is negative, her WBC is 9,000 (70% neuts, 28% lymphs, 2% bands), and her LP reveals a CSF WBC count of 8. BC, UC, and CSF cultures are sent. Acceptable management options for this child would include any one of the following except: • IM ceftriaxone in the ED • Admission to the hospital for IV antibiotics • Discharge with follow-up in 24 hours • Admission to the hospital for observation • Discharge on amoxicillin
Question 3 • A 19 month old boy comes to the ED with a 3 day history of fever. He appears well but his tympanic T is 39.8C. His chest is clear, his abdomen is soft, and he is circumcised. No source can be found for his fever. A CBC reveals a WBC of 8200 (60% neuts, 27% bands). BC’s are sent. Appropriate management at this point will be to: a. Obtain a urine sample b. Administer IM ceftriaxone c. Perform an LP d. Obtain a CXR e. Discharge on antipyretics
Objectives • Definitions • Which patients need in-depth evaluation and treatment? • What laboratory studies are indicated for various age ranges? • Which patients need treatment with antibiotics? • Which patients should be hospitalized?
Definitions • Fever • Fever without focus • Fever of unknown origin • Occult bacteremia • Serious bacterial infection (SBI)
What is fever? Rectal temperature > 38C, either at physician’s office, ED, or documented at home by a reliable parent or other adult
Different body sites • Rectal standard • Oral 0.5-0.6 lower • Axillary 0.8-1.0 lower • Tympanic 0.5-0.6 lower Documented: • In the absence of antipyretics • In ED or office or by hx from reliable parents/adults
Frequency of febrile illness • 35% of unscheduled ambulatory care visits • 65% of kids see doc before age 2y • Majority (75%) for T < 39 C • 13% T > 39.5
Fever of Unknown Origin 1. Fever of 38C or greater which has continued for a 2 to 3 weeks 2. Absence of localizing clinical signs 3. Negative simple investigations
Fever without focus • “An acute febrile illness in which the etiology of the fever is not apparent after a careful history and physical examination.” • 20% of childhood fevers have no apparent cause Baraffet al, Pediatrics 1993; 92:1-12
Occult bacteremia • “…a positive blood culture in the setting of well appearance and without focus (e.g. no pneumonia) • Fleisher et al, J Pediatrics 1994
Occult bacteremia organisms • Streptococcus pneumonia> 85% • Haemophilusinfluenzae type B (now rare – previously 10%) • Neisseriameningitidis3-5% • Others: • S. aureus • S. pyogenes (GAS) • Salmonella species
Outcomes of occult bacteremia without antibiotics • Persistent fever 56% • Persistent bacteremia 21% • Meningitis 9% • S. pneumonia 6% • H. Influenzae 26% (now rare)
Age is quite matter • >10 % of well-appearing young infants with a temperature >38°C has a serious bacterial infection or meningitis • Only <2 %of well-appearing older infants and young children with a temperature >39°C (manifest bacteremia
Serious Bacterial Infection • “…Include meningitis, sepsis, bone and joint infections, urinary tract infections, pneumonia and enteritis” Baraffet al, Pediatrics 1993; 92:1-12
Fever Practice Guidelines • CPS guidelines: Management of the febrile one-to 36-month-old child with no focus of infection. • Paediatr Child Health 1996;1:41-45 *re-affirmed April 2002 • “American” consensus guidelines: Practice guideline for the management of infants and children 0-36 months of age with fever without source. • Baraff et al, Pediatrics 1993;92:1-12
Case scenarios - fever • By age group: • < 1 month of age • 1 – 3 months • 3 – 36 months
Why according to age • Because in young infants there's a greater probability of serious bacterial infection so more aggressive approach to the evaluation and management of fever is warranted.
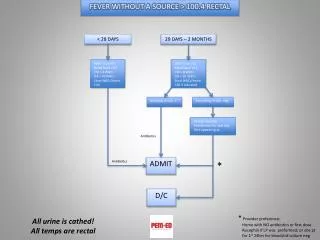
Febrile infant < 1 month “American” consensus recommendations • All should have: • Full septic w/u • CSF cultures, gm stain, cell count/diff, gluc/prot • Blood cultures • Urine routine, micro, culture • If diarrhea, stool exam (smear and culture) • If respsx: CXR • ADMIT, IV antibiotics, or • ADMIT, observe without antibiotics
Febrile infants 1-3 m of age According to validated criteria E.g. Rochester score • Low and high risk
Febrile infants < 3 months risk of bacteremia • If meets low risk Rochester 0.2% (1:500) criteria • If meets low risk criteria 0.7-1% but < 1 month
Febrile infants 1-3 m of age Hi Risk: “American” and Canadian Consensus recommendations • ADMIT to hospital with full septic w/u • BC, UC, LP • Broad-spectrum parental antibiotics
Febrile infants 1-3m of age low risk • Option 1 (“American”): Blood culture Urine culture LP Ceftriaxone 50 mg/kg IM Return for re-evaluation w/i 24 hours • Option 2 (“American” and CPS) No investigation (or urine culture only ) Careful outpatient observation, without treatment, close follow-up
Follow-up of Infants 1-3m old • Within 24 hours • Repeat exam for source, sequelae • Review, repeat labs • Arrange ongoing follow-up
Follow-up of 1-3m • If blood culture positive • ADMIT for sepsis evaluation • Parenteral antibiotics pending results • If urine culture positive • Persistent fever: ADMIT for sepsis evaluation and parenteral abx tx pending results • Afebrile and well: outpatient antibiotics
Fever Without SourceAge 3 – 36 Months • Risk of occult bacteremia • 3-11%, mean 4.3% for T>39C • Risk greater with • Higher temperatures • WBC > 15,000 (13%vs2.6%) • Risk of pneumococcal meningitis (w/o abxtx) 0.21% (1:500)
How should a child with FWF be evaluated? • Detailed history and thorough physical examination • avoid indiscriminately ordering a large battery of tests.
Physical examination:“Toxic appearance” • Lethargy/irritability • Poor/absent eye contact • Poor perfusion • Hypo/hyperventilation • Cyanosis
FWS – age 3-36 months:Consensus Recommendations • CHILD NON-TOXIC, T < 39C • No diagnostic tests or antibiotics • Acetaminophen 15 mg/kg prnfor fever • Return if fever persists > 48 hours or the followings happened:
Return to the Emergency Department if your child • more fussy or won’t stop crying • too sleepy or drowsy • stiff neck • Won’t stop vomiting • new rash • Has a seizure • Gets any other new or worsening symptom(s) that concerns you
FWS – age 3-36 months:Recommendations • CHILD NON-TOXIC, T 39C • Urine culture (for M < 6 month, F < 2 yrs age) • BC – 2 options • Option 1: obtain for all children with T 39C • Option 2: obtain if T 39C and WBC >15,000 • CXR, stool culture if indicated clinically • Acetaminophen 15 mg/kg q4h for T 39C • Follow-up in 24-48 hours *no antibiotics
FWS – age 3-36 months:Consensus Recommendations • CHILD APPEARS TOXIC: • ADMIT to hospital • Sepsis w/u • Parenteral abx
Investigation options [ ] CBC [ ] blood culture [ ] urinalysis [ ] urine culture [ ] CXR [ ] LP [ ] Nothing
Choice of antibiotic • If decide to treat empirically ceftriaxoneor poAmoxicillin/clavulanate
FWS – age 3-36 months:BC returns positive • Pneumococcus: • Persistent fever: ADMIT for sepsis w/u and parenteralabx pending sensitvity
FWS – age 3-36 months:BC returns positive • All Other Bacteria: • ADMIT for sepsis w/u and parenteralabx pending sensitivity results
FWS – age 3-36 months:Urine culture returns positive • All organisms: • ADMIT if febrile or ill-appearing • Outpatient abx if afebrile and well
Summary: FWS Infants < 28 days: Infants 1-3 months Non toxic children 3 m- 3 yrs (T <39C) Non toxic children 3 m-3 y(T 39C): Hospitalize +/- abx -According to risk score hospital Vs home, +/- abx Home, no antibiotics +/- labs, home, no antibiotics close follow-up in all!
No • risk for bacteremia • WBC • fever • male • age 7-11 mos ? "ill" , "toxic", "lethargic" Yes >20,000 WBC/mm3 ? ? ? Yes Consider Yes Hospital/ Antibiotic Rx AMOX or specify why other Toxic highly Febrile Child Aged 3-36 mos Without Apparent Focus Be Managed ? • Age 3-36 mos • Temp. > 390C Regardless of PCV status
“ I think it is clear that the handwriting is on the wall saying that occult bacteremia is dead. It was dying when Hib disappeared and Prevnar has destroyed it.” contribution to Pediatric Emergency Medicine List Serve
Heptavalent conjugate pneumococcal vaccine • very efficacious • Likely to make most of the foregoing pneumococcal in 3-36 month group obsolete • Finally become routine by MCH Given at 2,4,6 month and 12-15m
PCV7 2003 vs baseline 77% (<1 yr) 83% (1 yr) 64% (2 yr) Effect in Target Age Group Invasive Pneumococcal Disease Rates in Children < 3 Years, ABCs, 1998-2003 1 yr <1 yr 2 yrs 2003 data are preliminary Farely et al, ICP, Cancun, Mexico, August 2003
2003 vs baseline 77% (<1 yr) 83% (1 yr) 64% (2 yr) Effect in Target Age Group Invasive Pneumococcal Disease Rates in Children < 3 Years, ABCs, 1998-2003 ~ 80% in invasive pneumococcal disease in children < 3 yrs 2003 data are preliminary Farely et al, ICP, Cancun, Mexico, August 2003