Download
1 / 16
160 likes | 930 Views
Dermatomyositis Complicated by Pneumomediastinum and Subcutaneous Emphysema. Andrew Knerl, MD, (Associate) Cuong Doan, MD, (Member) Exempla Saint Joseph Hospital Denver, Colorado. Case Presentation. 29-year-old female 6 month history of dermatomyositis Heliotrope rash and biopsy

E N D
Dermatomyositis Complicated by Pneumomediastinum and Subcutaneous Emphysema Andrew Knerl, MD, (Associate) Cuong Doan, MD, (Member) Exempla Saint Joseph Hospital Denver, Colorado
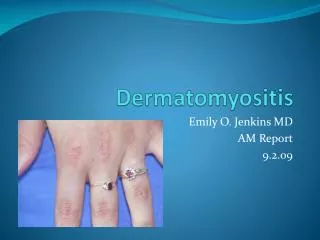
Case Presentation • 29-year-old female • 6 month history of dermatomyositis • Heliotrope rash and biopsy • Gottron’s patches • Later developed muscle weakness and vasculitic lesions • 1 month history of interstitial lung disease (ILD) • Based on CT scan from hospitalization for presumed PNA • Bronchoscopy with biopsies negative for PCP • Colonoscopy, EGD, CT abd/pelvis without evidence of cancer
Case Presentation • Treatment with prednisone, azathioprine, hydroxychloroquine, mycophenolate mofetil, and nifedipine • On admission: mycophenolate mofetil, hydroxychloroquine, prednisone, and nifedipine • Admitted to the hospital for neck pain and swelling • No difficulty breathing or swallowing
Exam findings • Crepitance over neck, chest, back and upper arms • Vasculitic lesions on hands and fingers • Ulcerations on fingertips • Labs unremarkable except for an elevated ESR and CPK
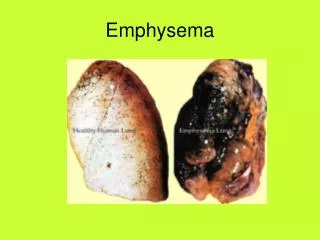
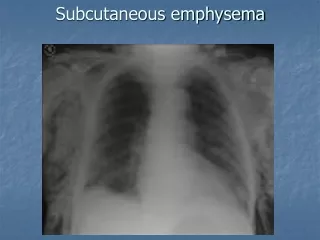
Radiology findings • Neck soft tissue x-ray: large subcutaneous air • CXR: subcutaneous emphysema • CT Neck: air tracking into the neck, the base of the skull, and the retropharyngeal space • CT Chest: pneumomediastinum extending into the neck, back, axilla, and spinal column • Etiology inapparent • Thin air around lungs, likely extrapleural • Contrast esophagram: no perforation
Hospital Course • Pulse dose steroids (1 g IV x 3 days) followed by prednisone 60 mg daily • Mycophenolate mofetil and hydroxychloroquine as WBC tolerated • No source of pneumomediastinum or subcutaneous air identified • Subcutaneous emphysema improved and the patient was discharged home to follow up with rheumatology and pulmonology • Meds: mycophenolate mofetil and prednisone
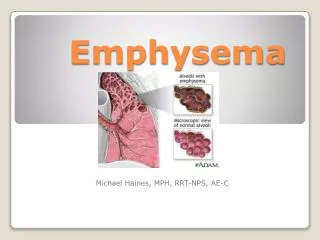
Dermatomyositis • Inflammatory myopathy characterized by a skin eruption that usually precedes muscle weakness
Dermatomyositis • Heliotrope rash on the upper eyelids with edema may be present • Gottron’s sign—an erythematous, raised, scaly eruption involving the knuckles, knees, and elbows
Dermatomyositis • Muscle weakness is a progressive, symmetric process that initially affects the proximal muscles • Pharyngeal muscles may be involved, resulting in dysphagia, and, in advanced cases, respiratory muscles may also be affected
Dermatomyositis and Malignancy • Increased incidence of ovarian ca, breast ca, melanoma, colon cancer, and NHL.
Dermatomyositis • Interstitial lung disease may precede the myopathy or occur early in the disease, and develops in 5-30% of patients • Pneumothorax, pneumomediastinum, and subcutaneous emphysema are rare complications of dermatomyositis-related ILD and carry a poor prognosis • A literature search by Kono et al in 2000 reported 13 cases of pneumomediastinum in the setting of dermatomyositis
Hypotheses • Rupture of subpleural blebs and dissection around perivascular sheaths • Vasculopathy causing subpleural infarctions and interstitial emphysema • Since pneumomediastinum is more common in patients with ulcerative or vasculitic lesions of the skin
Treatment Options • Limited evidence due to small number of reported cases • As an outpatient, was switched from mycophenolate mofetil to cyclophosphamide • Improvement to date with recent CXR showing resolved pneumomediastinum • Back at work and in the gym • Currently tapering prednisone and azathioprine • Vasculitic lesions and ulcerations have resolved
References • FaizFaiz, Saadia A. et al. “Dermatomyositis With Pneumomediastinum and Rapidly Progressing Interstitial Lung Disease.” Chest (2006). • Kono, Hajime et al. “Pneumomediastinum in Dermatomyositis: Association With Cutaneous Vasculopathy.” Annals of the Rheumatic Diseases 2000; 59:372-376. • Powell, Christian et al. “A 34-Year-Old Man With Amyopathic Dermatomyositis and Rapidly Progressive Dyspnea With Facial Swelling.” Chest 2007; 132:1710-1713.