Download
1 / 28
280 likes | 437 Views
Calcitonin in der klinischen Routine. M. Zimny. Calcitonin (Polypeptid mit 32 Aminosäuren) . nachweisbar bei Wirbeltieren bei Säugetieren Produktion in den C-Zellen der Schilddrüse entdeckt 1962 von Copp als “hormone in search of a function”

E N D
Calcitonin in der klinischen Routine M. Zimny
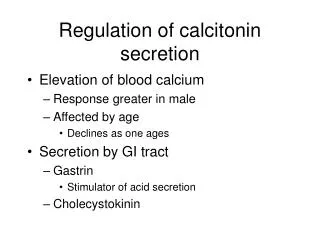
Calcitonin (Polypeptid mit 32 Aminosäuren) • nachweisbar bei Wirbeltieren • bei Säugetieren Produktion in den C-Zellen der Schilddrüse • entdeckt 1962 von Copp als “hormone in search of a function” • hemmt Osteoklasten, fördert die Einlagerung von Calciumphosphat in das Osteoid, Anstieg im Serum nach Calcium-load • physiologische Bedeutung beim Menschen und Säugetieren unklar (normale Ca++-Konzentration ohne messbare Calcitoninspiegel, kann erhöhte Ca++-werte bei HPT nicht verhindern)
Calcitonin • HWZ im Serum 4,5h - 26h, Ardoillou 1970 • verlängerte HWZ bei Leber-, Pankreas-, Niereninsuffizienz (Henriksen 2000) • im Blut nachweisbar hCT-Monomere, Dimere, Vorstufen und Abbauprodukte • Analyse der Monomere über “Sandwich-Assay” (IRMA, z.B. Medipan Calcitonin magnum) unter Verwendung monoklonaler AK - keine Kreuzreaktivität mit Calcitonin anderer Spezies (Lachs)
Calcitonin - (Prä)-Analytik • Abnahme in Serumröhrchen • nach Geringung zentrifugieren • - bis zur Analyse bei -20° einfrieren • Zugabe des Signal-AK (125J) • Inkubation > 18h • Zugabe des Capture-AK (kalt) • Inkubation 2h • Zugabe Magnet-Immunosorbents • Magnettrennung • Messung
Epitop II Epitop I Tracer (125J-monokl. Maus-AK) Antiserum (polyklonaler Kaninchen AK) hTC Immunosorbent (Magnetpartikel) • High dose hook > 100000 pg/ml • funkt. Assay-Sensitivität = 1,5 pg/ml • Normwerte : f < 10 pg/ml m < 15 pg/ml f < 2,9 pmol/l m < 4,35 pmol/l
Calcitonin • Erhöht bei C-Zell-Proliferation (CCH, MTC) • paraneoplastische Erhöhung bei BC, seltener Mamma-Ca, Magen-Ca • verlängerte HWZ bei Niereninsuffizienz, Leberinsuffizienz • erhöhte Werte unter Protonenpumpeninhibitoren • erhöhte basale und stimulierte Calcitonin-Spiegel bei Pseudohypoparathyreoidismus
Pentragastrin-Stimulations-Test • langsame i.v. Injektion von 0,5µg / kgKG Pentagastrin (Peptavlon®, SERB S.A. Paris, Frankreich) • Blutentnahme bei 0, 2, 5, 10 min pathologisch: Anstieg > 100 pg/ml grenzwertig: Anstieg 30 - 100 pg/ml negativ: Anstieg < 30 pg/ml NW: Übelkeit/Erbrechen, Magenschmerzen, sternaler Druck... Probleme: Verfügbarkeit, Finanzierung,
Alternativen? Omeprazol (2x20 mg über 4 Tage) • Omeprazol stimuliert endogene Gastrinsekretion • Gastrinstimulus sehr variabel, Calcitoninanstieg niedriger als unter Pentagastrin, Trennschärfe schlechter als bei Pentagastrintest (Vitale 2002 Clin Chem). Calciuminfusion (ca. 3mg/kg/4h) Whiskey (Dosierung unbekannt) • geringerer Calcitonin-Anstieg als nach Pentagastrin(Emmertsen 1980)
Prognose SD-CA in Abhängigkeit von der Histologie (Hundahl Cancer 1998)
Hintergrund • Operation einziger curativer Ansatz bei medullärem Schilddrüsenkarzinom • Tumorstadium entscheidender prognostischer Faktor (I = 100%, II = 90%, III = 87%, IV = 56% 5- Jahresüberlebensrate (Kebebew Cancer 2000) • LK-Metastasen häufig schon bei Tumoren < 1cm (33-67%, Scollo JCEM 2003) • biochemische Heilung bei N0 100%, vs. 33% bei N1 (Gimm 1998)
Häufigkeitsverteilung SD-Ca in Deutschland (Hölzer Cancer 2000) und in Hanau
Ergebnisse Calcitonin-Screening Autor Jahr CT Cutoff (pg/ml) MTC Pacini 1994 8/1385 20 8/8 Vierhapper 1997 72/1062 5 6/72 Niccoli 1997 34/1167 10 14/34 Karanakis 2004 28/414 10 1/28 Pacini 2004 47/10864 20 44/47 Constante 2007 ?/5817 15/? Hanau 2007 885/21928 10 28/369 basal CT : 0,4 - 6,9% MTC bei basal CT : 3,5 - 100% MTC im Kollektiv : 0,13 - 1,2%
Prädiktiver Wert der präoperativen Calcitoninbestimmung (Costante JCEM 2007)
Problem neoplastische / nicht neoplastische C-Zell Hyperplasie
CCH selten bei Frauen - CT prädiktiver für MTC als bei Männern
Trennschärfe - Calcitonin (basal / stimuliert) stimuliert basal
Trennschärfe - Calcitonin (basal / stimuliert) stimuliert basal
Autoimmunthyreoiditis - Calcitonin • 1 MTC bei 568 Pat. Mit AIT ohne Knoten (Schütz 2006)
Prävalenz AIT bei Patienten mit MTC Prävalenz AIT im Geasmtkollektiv
Zusammenfassung • MTC ist selten • Calcitonin-Screening ist sensitiv, entdeckt MTC im frühen, pot. curablen Stadium • prädiktiver Wert für basales / stimuliertes Calcitonin limitiert (PPV 4-67%) • sichere Unterscheidung MTC / CCH gelingt nicht • 20% AIT bei MTC vs.12-16% im Gesamtkollektiv • kein Zusammenhang CT und TPO-AK • CCH bei Frauen selten