Download
1 / 41
410 likes | 1.24k Views
Blood pressure. “This may be the most important number we encounter during our day.” – Dr Mark Johnson. August 11 th 2010. Hypertension. Wednesday morning map of hypertension:

E N D
Blood pressure. “This may be the most important number we encounter during our day.” – Dr Mark Johnson August 11th 2010
Hypertension Wednesday morning map of hypertension: 8/10: Management of HTN in outpatient setting: home BP monitoring, using your MD, RN team, symptom evaluation and triage over the phone, lab monitoring 12/8: Benchmarks, pay for performance standards, interval between visits, follow up guidelines. 6/8/11: Preventive medicine: age based screening recommendations Didactics: 8/17 treatment of hypertension, identification and treatment of secondary hypertension, use of labs and studies
Goals for this morning • With regard to elevated blood pressure, what are the key features of a clinic visit? • what is in the number • making a diagnosis • What is the best way to monitor elevated blood pressure? • ambulatory monitoring • home BP monitoring • using the multidisciplary team • patient self directed goals 3. What is involved in phone triage for blood pressure concerns? • What symptoms are useful 4. What are the goals of care?
THE VISIT- you see that important number on the chart and… …you think Is that one number important? Is that number accurate? What is next in the care of this patient?
One number? AHA made a summary of recommendations in 2005 It is better to have more than one number to switch your mindset from “screening” to “evaluation” of elevated blood pressure. At the first visit: • blood pressure should be measured in both arms • at least two readings with a 1 minute interval between • additional readings if the difference is > 5 mm Hg.
One number IS useful when> 180/120 Hypertensive urgency BP >180/120 without evidence of end-organ dysfunction. (Headaches, dyspnea, epistaxis or anxiety do not count.) Hypertensive emergency >180/120 with end organ dysfunction cerebrovascular: encephalopathy, intracerebral hemorrhage cardiac: acute dissection, acute LV failure, acute or impending MI ocular: retinal hemorrhages, papilledema renal: acute glomerulonephritis or acute nephropathy. Other emergencies: eclampsia, cocaine use, rebound HTN after stopping antihypertensive agents, pheochromocytoma crisis Malignant hypertension: (same as above)
How many numbers? AHA recommendations: • Unless profoundly elevated or symptomatic, the diagnosis of HTN shouldn’t be made on the first visit • Diagnose after greater than three readings spaced over a period of weeks to months • 1 in 3 patients who appear to have mild hypertension on a first visit to a new doctor, will have normal blood pressure by the 6th visit USPSTF: recommendations • Diagnose after greater than two readingsspaced over at least 2 visits over a period of 1 to several weeks.
Accurate number? American Heart Association Guidelines for In-Clinic Blood Pressure Measurement Recommendations Us of a sphygmomanometer is ideal Patient should be seated comfortably, with back supported, legs uncrossed, and upper arm bared. • Diastolic pressure is higher in the seated position, whereas systolic pressure is higher in the supine position. An unsupported back may increase diastolic pressure; crossing the legs may increase systolic pressure. Patient’s arm should be supported at heart level. • If the upper arm is below the level of the right atrium, the readings will be too high; if the upper arm is above heart level, the readings will be too low. If the arm is unsupported and held up by the patient, pressure will be higher. Cuff bladder should encircle 80 percent or more of the patient’s arm circumference. • An undersized cuff increases errors in measurement. Mercury column should be deflated at 2 to3 mm per second. • Deflation rates greater than 2 mm per second can cause the systolic pressure to appear lower and the diastolic pressure to appear higher.
THE VISIT- you see that important number… …you think Is that one number important? yes if > 180/120 yes, if < 180/120 it is the beginning of the evaluation no it does not make a diagnosis of hypertension Is that number accurate? was the blood pressure taken in both arms, in the proper manner? were two readings with a one minute interval between them? What is the next in the care of this patient?
History*: History of previous hypertension Drug use: amphetamines, cocaine, PCP Medication review prescription and non prescription Adherence to BP medications, time from last dose *use of sildenafil Exam*: BP both arms, proper size cuff, proper technique fundoscopic exam murmurs/gallops pulmonary edema bruits AAA pulses in all extremities mental status exam Key elements of the visit *most high yield
Initial evaluation Labs/studies: Electrolytes (K, Na, Ca, Cr) UA hct EKG Urine tox screen TSH Based on clinical evaluation: imaging as indicated by exam * hospitalization/ cardiac evaluation/monitoring
THE VISIT Thoughts for extra credit What patients should you think about secondary hypertension?
THE VISIT ends- …you now have several blood pressures, a good history and physical and some labs and studies ordered You have thought- Is that one number important? Is that number accurate? What is next in the care of this patient? • we need more numbers…at least 2 or three over time • there are different ways of collecting these numbers
THE VISIT ENDSbut the blood pressure remains Ambulatory monitoring readings are taken every 15 to 30 minutes for 24 hours Indications (Medicare approved 2005) • Episodic hypertension • Suspected autonomic neuropathy • Suspected over-treatment & iatrogenic hypotension • Significant discrepant readings between home and clinic
THE VISIT ENDSbut the blood pressure remains Home blood pressure monitoring A patient is asked to take their blood pressure at different times of the day 2-3 times/week. Rationale: • May be more accurate predictor of morbidity than clinical readings • Better ability to manage treatment for older patients, risk for hypotension. May aid medication dosing decisions • Selected devices have passed proper validation tests. • Upper arm only • Automated devices in the community in public retail areas, little info on accuracy. • Fire department offers free BP readings • Stay tuned: Barbershops may be useful places for monitoring high blood pressure in African-American men in United States, based on 2 nonrandomized feasibility studies. Hypertension 2007 May;49(5):1040)
THE VISIT ENDSbut the blood pressure remains Should we ask our patients to monitor their BP? Yes: TASMINH2 trial (Lancet 2010 Jul 17;376 a randomized trial • 527 patients aged 35-85 years with blood pressure > 140/90 mm Hg receiving antihypertensive therapy randomized to self-management vs. usual care • self-management self-titration of antihypertensive drugs, self-monitoring of blood pressure, plus telemonitoring of blood pressure measurements • mean systolic blood pressure with self-management vs. usual care • -12.9 mm Hg vs. -9.2 mm Hg at 6 months (p = 0.013) • -17.6 mm Hg vs. -12.2 mm Hg at 12 months (p = 0.0004)
THE VISIT ENDSbut the blood pressure remains Should we ask our patients to monitor their BP? Maybe not: (BMJ 2005 Sep 3;331(7515):493 441 primary care patients with hypertension > 140/85 mm Hg were randomized to practice-based self-monitoring vs. usual care (blood pressure monitored by practice) (No self titration of medications) Practice-based self-monitoring reduced systolic blood pressure by 4.3 mm Hg at 6 months (95% CI 0.8-7.9 mm Hg) and 2.7 mm Hg at 1 year (not statistically significant)
what is next? You have the patient follow up in intervals ranging from 2-6 weeks for 1-3 visits. You have accurate blood pressures obtained over weeks to months. You can now: 1. Make a diagnosis 2. Educate your patient 3. Develop a self management plan using your multidisciplinary team.
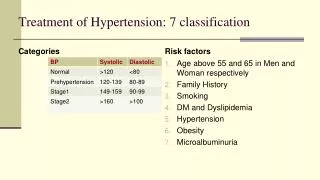
Make a diagnosis We use the number to diagnose and code: JNC 7 Normal SBP < 120 and DBP < 80 Pre hypertension 120-139 or DBP 80-90 Stage I hypertension SBP 140-159 or DBP 90-99 Stage II hypertension SBP 160-179 or DBP 100-119
Make a diagnosisin a child stage 1 hypertension 95th% - 99th% plus 5 mm Hg, based on charts for gender, age and height stage 2 hypertension > 99th% plus 5 mm Hg, based on charts for gender, age and height Pediatrics 2004 Aug;114(2 Suppl 4th report):555
TABLE 1 Blood Pressure Values Requiring Further Evaluation, According to Age and Gender4,6 Pediatrics 2009 Jun;123(6):e972 My memory aid: Search deep into coat pocket for children’s guide if: Age ~5: > 100/60 Age ~10: > 110/70 Age ~15: > 120/75
Make a diagnosis in a child. • Unless profoundly elevated or symptomatic, a child should not be diagnosed with hypertension on the first visit • Measure leg blood pressure • The right arm is always preferable for consistency and comparison with reference tables • After 3-6 readings spaced over a period of weeks to months, hypertension can be diagnosed while evaluationis underway
Our goals: lower our patient’s blood pressure to < 140/90 in most cases help prevent end organ disease adhere to pay for performance standards Patient goals: lessen symptoms reduce risk of future life impairment decrease fears help others with the same condition - many others Pause, be attentive to your goals (versus?) the patient’s health There are many organizations whose work is dedicated to improving outcomes using a patient centered approach to treatment of chronic disease.
Team based careperspective #1 Institute for Healthcare Improvement IHI Organization founded in early 1990s, non profit to help improve and standardize quality care. Patient self management protocols helps instruct many of the successful clinic based quality improvement projects in chronic disease
IHI -Self management principles Patients with chronic illness need support, as well as information to become effective mangers of their own health. Essentials: • Basic information about their disease • Assistance with self-management skill building • Ongoing support from members of the practice team, family, friends and community.
IHI-principles of the care team Use techniques that emphasize patient activation or empowerment, collaborative goal setting Be sensitive to the role that families, caregivers, and communities play in different cultures. The provider team can use assessments of patient self-management to enhance its ability to support patients. Assessments include questions about knowledge, skills, confidence, supports, and barriers.
IHI-principles of patient education Importance of high quality patient education materials Assess for language and cultural appropriateness (different versions may be necessary to serve patients.) Make materials available to patients, families, providers (waiting rooms, exam rooms, AVS)
IHI- put into practice Identify a self-management tool such as: • An action plan that includes goals and describes behavior i.e. increasing activity by walking 15 min 3x/week including a follow up plan • Review the plan with the multidisciplinary team • Assign roles--who has the responsibility for each step of the planned visit • Review goals with patients as part of the planned follow up • This will include assessment of the patients’ skill, understanding and confidence in managing their disease • Give the patient a copy of goals • Establish a leader • Modify the use of the tool and to train new members of the team
Team based careperspective #2 The Cochrane Collaboration An international, independent, non-profit organization whose mission is it to provide evidence based information on the effects of healthcare. Cochrane 2006 Issue 4:CD005182 Systematic review of 56 randomized trials of interventions to improve blood pressure
Cochrane 2006, improvement of blood pressure Key points: • Organized system of regular review linked to vigorous antihypertensive drug therapy reduced blood pressure by 8-12/4-8 and all cause mortality at 5 years, NNT 72. • Self-monitoring reduced blood pressure • Appointment reminders increased proportion of patients to attended follow up • Educational interventions alone unlikely to provide large effects on blood pressure • Nurse- or pharmacist-led care improved blood pressure control in most but not all trials • Follow-up every 6 months for stable hypertension is adequate.
Subsequent visits Symptom evaluation Laboratory monitoring: after diuretic initiation check K within 2-8 weeks patients with renal insufficiency or heart failure should have labs 2-8 weeks after initiation then q 3 months patients with stable hypertension labs q 6 months Adjust medications: every 6 weeks, no benefit sooner than that. Review home blood pressure readings More to follow in subsequent didactic sessions.
Subsequent visits Address patient self management goals using tools and multidisciplinary care team Patient education Make plans for follow-up support Send reminder letters
Care coordination Dedicated time to care for patients outside of a clinic visit This may include follow up with treatment recommendations Triaging symptoms Making medication changes using home blood pressure monitoring Enquiring about barriers to care, questions that arise.
hypertensive urgencies headache in 22% epistaxis in 17% faintness in 10% psychomotor agitation in 10% chest pain in 9% dyspnea in 9% vertigo in 7% paresthesia in 6% arrhythmia in 6% neurologic deficit in 3% vomiting in 2% hypertensive emergencies chest pain in 27% dyspnea in 22% neurologic deficit in 21% faintness in 10% paresthesia in 8% headache in 3% vertigo in 3% vomiting in 3% Symptom triage Based on a study of 449 patients with hypertensive crisis presenting to ED. Published 1996.
Goals revisited What is the best technique for obtaining blood pressure? What is hypertensive emergency and what are the key signs and symptoms? What are the key parts of the history and physical when concerned about hypertension? Consider indications for assessing for secondary hypertension.
Goals revisited What are the initial studies worth doing? Indications for ambulatory blood pressure monitoring? Consensus on home blood pressure monitoring? What are some of the key principles of patient self management?
Goals revisited What might you ask over the phone to triage concerning hypertension? Should you let a person drive professionally if they have hypertension? If BP 160-180/90-105 temporary certification may be given for 3 months to allow time for driver to be evaluated and treated If BP > 180/105, driver should not be certified and with treatment should only be certified for 1 year at a time; disqualification recommended if significant target organ damage which increases risk of sudden collapse
Go forth to the teams and create self management tools and protocols and become excited about these important patients… and their numbers. Thank you.