Download
1 / 64
670 likes | 1.3k Views
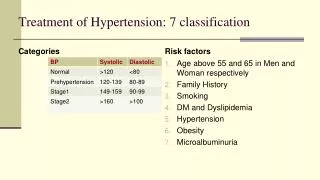
Treatment of Hypertension: 7 classification. Categories. Risk factors. Age above 55 and 65 in Men and Woman respectively Family History Smoking DM and Dyslipidemia Hypertension Obesity Microalbuminuria. Treatment of Hypertension – . 7 compelling Indications : Heart failure

E N D
Treatment ofHypertension: 7 classification Categories Risk factors Age above 55 and 65 in Men and Woman respectively Family History Smoking DM and Dyslipidemia Hypertension Obesity Microalbuminuria
Treatment of Hypertension – • 7 compelling Indications: • Heart failure • Coronary artery disease • H/o MI • H/o stroke • Diabetes • Chronic Renal failure
Treatment of Hypertension – General principles • Stage I: • Start with a single most appropriate drug with a low dose. Preferably start with Thiazides. Others like beta-blockers, CCBs, ARBs and ACE inhibitors may also be considered. CCB – in case of elderly and stroke prevention. If required increase the dose moderately • Partial response or no response – add from another group of drug, but remember it should be a low dose combination • If not controlled – change to another low dose combination • In case of side effects lower the dose or substitute with other group • Stage 2: Start with 2 drug combination – one should be diuretic
Treatment of Hypertension – combination therapy • In clinical practice a large number of patients require combination therapy – the combination should be rational and from different patterns of haemodynamic effects • Sympathetic inhibitors (not beta-blockers) and vasodilators + diuretics • Diuretics, CCBs, ACE inhibitors and vasodilators + beta blockers (blocks renin release) • Hydralazine and CCBs + beta-blockers (tachycardia countered) • ACE inhibitors + diuretics • 3 (three) Drug combinations: CCB+ACE/ARB+diuretic; CCB+Beta blocker+ diuretic; ACEI/ARB+ beta blocker+diuretic
Treatment of Hypertension. • Never combine: • Alpha or beta blocker and clonidine - antagonism • Nifedepine and diuretic synergism • Hydralazine with DHP or prazosin – same type of action • Diltiazem and verapamil with beta blocker – bradycardia • Methyldopa and clonidine • Hypertension and pregnancy: • No drug is safe in pregnancy • Avoid diuretics, propranolol, ACE inhibitors, Sodium nitroprusside etc • Safer drugs: Hydralazine, Methyldopa, cardioselective beta blockers and prazosin
Treatment guidelines (ESH/ESC 2007) Average risk Low added risk Moderate added risk High added risk Very high added risk ESH – ESC Guidelines Committee. J Hypertens 2007; 25: 1105–1187
Complications of Hypertension:End-Organ Damage Hypertension Hemorrhage, Stroke LVH, CHD, CHF Peripheral Vascular Disease Renal Failure, Proteinuria Retinopathy CHD = coronary heart disease CHF = congestive heart failure LVH = left ventricular hypertrophy Chobanian AV, et al. JAMA. 2003;289:2560-2572.
Conditions favouring the use of some antihypertensive drugs versus other • Subclinical organ damage: LVH ACEI, CA, ARB Asymptomatic Atherosclerosis CA, ACEI Microalbuminuria ACEI, ARB Renal dysfunction ACEI, ARB
Conditions favouring the use of some antihypertensive drugs versus other • Clinical event: Previous stroke any BP lowering agent Previous MI BB, ACEI, ARB Heart failure diuretics, BB, ACEI, ARB, anti-aldosterone agents Tachyarrhythmias BB Periph.art.disease CA LV dysfunction ACEI
Conditions favouring the use of some antihypertensive drugs versus other • Condition : ISH (elderly) diuretics,CA Metabolic syndrome ACEI,ARB,CA Diabetes mellitus ACEI, ARB Pregnancy CA,methyldopa,BB Glaucoma BB
Monotherapy versus combination therapy • Monotherapy allows to achieve BP target only in a limited number of patients • Use of more than one agent is necessary to achieve target BP • Initial therapy: monotherapy or combination of two drugs in low doses with subsequent increase in drug doses or number
Monotherapy versus combination therapy • Monotherapy in mild BP elevation with low or moderate total CV risk • Two drugs at low doses should be preferred as the first step when BP is in grade 2 or 3 or total CV risk is high or very high with mild hypertension • Fixed combination of two drugs simplify the treatment • If BP control is not achieved by two drugs, combination of three or more drugs is required
Possible combinations of different classes of antihypertensive agents Diuretics AT1-receptorblockers β-blockers CCBs α-blockers ACE, angiotensin-converting enzyme AT, angiotensin CCB, calcium-channel blocker ACEinhibitors The preferred combinations in general hypertensive population are represented as thick lines. The frames indicate classes of agents proven to be beneficial in controlled interventional trials ESH – ESC Guidelines Committee. J Hypertens 2007; 25: 1105–1187
Antihypertensive therapy in special groups • Elderly patients • Diabetic patients • Patients with renal dysfunction • Patients with cerebrovascular disease • Patients with coronary heart disease and heart failure • Patients with atrial fibrillation
Beta-adrenergic blockers • Non selective:Propranolol (others: nadolol, timolol, pindolol, labetolol) • Cardioselective: Metoprolol (others: atenolol, esmolol, betaxolol) • All beta-blockers similar antihypertensive effects – irrespective of additional properties • Reduction in CO but no change in BP initially but slowly • Adaptation by resistance vessels to chronically reduced CO – antihypertensive action • Other mechanisms – decreased renin release from kidney (beta-1 mediated) • Reduced NA release and central sympathetic outflow reduction • Non-selective ones – reduction in g.f.r but not with selective ones • Drugs with intrinsic sympathomimetic activity may cause less reduction in HR and CO
Beta-adrenergic blockers • Advantages: • No postural hypotension • No salt and water retention • Low incidence of side effects • Low cost • Once a day regime • Preferred in young non-obese patients, prevention of sudden cardiac death in post infarction patients and progression of CHF • Drawbacks (side effects): • Fatigue, lethargy (low CO?) – decreased work capacity • Loss of libido – impotence • Cognitive defects – forgetfulness • Difficult to stop suddenly • Therefore cardio-selective drugs are preferred now
Beta-adrenergic blockers • Advantages of cardio-selective over non-selective: • In asthma • In diabetes mellitus • In peripheral vascular disease • Current status: • JNC 7 recommends - 1st line of antihypertensive along with diuretics and ACEIs • Preferred in young non-obese hypertensive • Angina pectoris and post angina patients • Post MI patients – useful in preventing mortality • In old persons, carvedilol – vasodilatory action can be given
Adrenergic ReceptorsReview of ANS • Sympathetic Nervous System • Alpha 1 = vasoconstriction • Alpha 2 = feedback/vasodilation • Beta 1 = increases heart rate • Beta 2 = bronchodilation
Beta Adrenergic Blocking Agents • Known as Beta-blockers • Axn: Inhibit cardiac response to sympathetic nerve stimulation by blocking Beta receptors • Decreases heart rate and C.O. • Decreases blood pressure
Beta Adrenergic Blocking Agents • Examples – “olol” names • Beta 1: Atenolol • Beta 1 and 2: Propranolol
Nursing Implications • Can not be abruptly discontinued • Check baseline b.p. • Check hx. of resp. condition-aggravates bronchoconstriction
Side effects • Bradycardia • Bronchospasm, wheezing • Diabetic: hypoglycemia • Heart failure: edema,dyspnea,rhales
DIURETICS • MOA: • 1- ↑ renal excretion of Na & water ↓ plasma volume ↓ C.O. • 2- ↓ peripheral resistance ( desensitize smooth muscles to action of catecholamines )
1-Thiazide • Sulfonamide molecule • Prolonged action • Flat curve response • Potentiates action of other anti HTN • Eg: Hydrochlorothiazide ( Ezidrex ) , Bendrofluazide • SE: hypo K+ , hypo Na+, hyperuricemia, hyperglycemia, lipid profile disturb.
2- Loop Diuretics • Steep curve response • Restricted to CCF & CRF • Eg: Frusemide • SE: ↓ K+ , ↓ Na+ , hypotension, ototoxic in v.high doses
3- K+ sparing diuretics • Not effective alone, so used in combination • Eg: Spironolactone, Amiloride , Uniretic( HCT + Amiloride) • SE: ↑ K+, gynecomastia
Beta Blockers • MOA: • Block beta receptors ↓sympathetic drive • 1- ↓ H.R. & contractility, ↑ P.R. ↓ C.O. • 2- ↓ Renin release & activity ↓ Ang II ↓BP Act as anti HTN within 3-7 days
Beta Blockers • Metabolism: Hydroxylated in liver to water soluble compounds excreted in kidneys • Preferred in HTN with angina, SVT, HOCM, Thyrotoxicosis, Pheochromocytoma, Migraine and L.cirrhosis.
Beta Blockers • SE: bradycardia, bronchospasm, cold extremeties, hypoglycemia, insomnia, bad dreams • Overdose: hypotension, bradycardia, bronchospasm, coma ( treated with Atropine, Isoprenaline, glucagon ) • C.I: HF, Asthma, DM, H.Block, Periph.vascular diseases , Hyperlipidemia
Beta Blockers • Atenolol: less lipid soluble less CNS SE • Timolol: lipid soluble more CNS SE.
Thiazides • Mechanism of action: • = lower blood pressure by reduction of blood volume and by direct • vascular effect • inhibition of sodium chloride transport in the early segment of the distal • convoluted tubule natriuresis, decrease in preload and cardiac • output - renal effect • slow decrease of total peripheral resistance (raised initially) during • chronic treatment, suggesting an action on resistance vessels - • extrarenal effects • compensatory responses to pressor agents including angiotensin II and • noradrenaline are reduced during chronic treatment with thiazides • used with loop diuretic - synergistic effect occurs
Thiazides Adverse effects: - Idiosyncratic reactions (rashes - may be photosensitiv, purpura) - Increased plasma renin (which limits the magnitude of their effect on BP) - Metabolic and electrolyte changes Hyponatremia Hypokalemia (combine with potassium-sparing diuretics) Hypomagnesemia Hyperuricemia(most diuretics reduce urate clearance) Hyperglycemia Hypercalcemia (thiazides reduce urinary calcium ion clearance precipitate clinically significant hypercalcemia in hypertensive patients with hyperparathyroidism) Hypercholesterolemia (a small in plasma cholesterol concentration)
LOOP DIURETICS furosemid - useful in hypertensive patients with moderate or severe renal impairment, or in patients with hypertensive heart failure. - relatively short-acting (diuresis occurs over the 4 hours following a dose) used in hypertension if response to thiazides is inadequate Mechanism of action: - they inhibit the co-transport of Na+, K+ and Cl- - of Ca2+ and Mg2+ excretion - they have useful pulmonary vasodilating effects (unknown mechanism)
LOOP DIURETICS Toxicity: - hypokalemic metabolic alkalosis (increased excretion of K+) - ototoxicity (dose dependent, reversible) - decrease of Mg2+ plasma concentration (hypomagnesemia) - hyperuricemia (competition with uric acid about tubular secretion) - sulfonamide allergy - risk of dehydration (> 4 L urine/ 24 h) Imporatant drug interaction may occurs if loop diuretic is given with Li+ (thymoprofylactic drug). Decrease of Na+ reabsorption can lead to increase of Li+ reabsorption toxicity.
b -adrenoreceptor antagonists • Mechanism of action: • the fall in cardiac output BP • - theyreduce renin secretion • CNS-effects ??? • additional mechanisms involve baroreceptors or other homeostatic • adaptations • Possible mechanisms include: • b-adrenoceptors located on sympathetic nerve terminals can promote • noradrenaline release, and this is prevented by b-receptor • antagonists • local generation of angiotensin II within vascular tissues is stimulated • by b2-agonists.
b-adrenoreceptor antagonists cardio-selective: b1blockersatenolol, metoprolol b1blockers with ISAacebutol b1 + a1blockerslabetalol, carvedilol cardio non-selective: b1 + b2blockersmetiprolol, propranolol, nadolol b1 + b2blockers with ISApindolol, bopindolol Note: Partial agonist activity (intrinsic sympathomimetic activity – ISA) - may be an advantage in treating patients with asthma because these drugs will cause bronchodilation; they have moderate (lower) effect on lipid metabolism, cause lesser vasospasms and negative inotropic effect
b-adrenoreceptor antagonists • Adverse effects • Cardiovascular adverse effects, which are extension of the beta • blockade, include: • bradycardia • antrioventricular blockade • congestive heart failure (unstable) • asthmatic attacks(in patients with airway disease) • premonitory symptoms of hypoglycemia from insulin overdosage • (eg, tachycardia, tremor and anxiety, may be marked) • CNS adverse effects - sedation, fatigue, and sleep alterations.
Hypertension & regulation of blood pressure Baroreflexes (mediated by autonomic nerves) Humoral mechanisms (include: RAAS system and local release of hormones from vascular endothelium, such as, NO, endothelin 1) Anatomic sites of blood pressure control
Hypertension & regulation of blood pressure A. Postural baroreflex: responsible for rapid , moment to moment adjustments in blood pressure. • Sense the stretch of the vessel walls • from a reclining to an upright posture; • reduction of peripheral vacular resistance; • Reduction in intravascular volume; -
Hypertension & regulation of blood pressure B. Renin-Angiotensin-Adolsteron (RAAS) Angiotensin II Redistribution of renal blood flow This is responsible for long-term blood pressure control.
I. Basic pharmacology of antihypertension agents 1. Diuretics:depleting the sodium and reducing blood volume and perhaps by other mechanisms. 2. Sympathoplegic agents:reducing peripheral vascular resistance, inhibiting cardic output, increasing venous pooling. 3. Direct vasodilators:relaxing vacular smooth muscle, dilaing resistance vessels and/or increasing capacitance. 4. Agents that block RAAS:reduce peripheral vacular resistance and blood volume.
1. Diuretics • Sodium restriction is very preventive in the control of blood pressure. It is a nontoxic and therapeutic measure. 1) Pharmacological roles (1) Diurectic action: In the early stage: reducing blood volume and cardiac output; In the late stage: reduce peripheral vascular resistance (by reducing the Na+; reduce Na+-Ca2+ exchange in vascular smooth muscle cells (Ca2+i , peripheral resistance ) (2) Non diurectic action: direct vasodilating, e.g. Indapamide, a non-thiazide sullfonamide diuretic with both diuretic and vasodilator activity; Amiloride inhibits smooth muscle responses to contractile stimuli.
Diuretics • Drugs causing net loss of Na+ and water in urine • Mechanism of antihypertensive action: • Initially: diuresis – depletion of Na+ and body fluid volume – decrease in cardiac output • Subsequently after 4 - 6 weeks, Na+ balance and CO is regained by 95%, but BP remains low! • Q: Why? Answer: reduction in total peripheral resistance (TPR) due to deficit of little amount of Na+ and water (Na+ causes vascular stiffness) • Similar effect is seen with sodium restriction (low sodium diet)
Thiazide diuretics – adverse effects • Adverse Effects: • Hypokalaemia – muscle pain and fatigue • Hyperglycemia: Inhibition of insulin release due to K+ depletion (proinsulin to insulin) – precipitation of diabetes • Hyperlipidemia: rise in total LDL level – risk of stroke • Hyperurecaemia: inhibition of urate excretion • Sudden cardiac death – tosades de pointes (hypokalaemia) • All the above metabolic side effects – higher doses (50 – 100 mg per day) • But, its observed that these adverse effects are minimal with low doses (12.5 to 25 mg) - Average fall in BP is 10 mm of Hg
Thiazide diuretics – current status • Effects of low dose: • No significant hypokalaemia • Low incidence of arrhythmia • Lower incidence of hyperglycaemia, hyperlipidemia and hyperuricaemia • Reduction in MI incidence • Reduction in mortality and morbidity • JNC recommendation: • JNC recommends low dose of thiazide therapy (12.5 – 25 mg per day) in essential hypertension • Preferably should be used with a potassium sparing diuretic as first choice in elderly • If therapy fails – another antihypertensive but do not increase the thiazide dose • Loop diuretics are to be given when there is severe hypertension with retention of body fluids