Download
1 / 97
1.01k likes | 1.56k Views
Injuries of the Clavicle, Acromioclavicular Joint and Sternoclavicular Joint. Andrew H. Schmidt, M.D. T.J. McElroy Created March 2004; Revised January 2007. Clavicle. “S”-shaped bone Medial - sternoclavicular joint Lateral - acromioclavicular joint and coracoclavicular ligaments

E N D
Injuries of the Clavicle, Acromioclavicular Joint and Sternoclavicular Joint Andrew H. Schmidt, M.D. T.J. McElroy Created March 2004; Revised January 2007
Clavicle • “S”-shaped bone • Medial - sternoclavicular joint • Lateral - acromioclavicular joint and coracoclavicular ligaments • Muscle attachments: • Medial: sternocleidomastoid • Lateral: Trapezius, pectoralis major
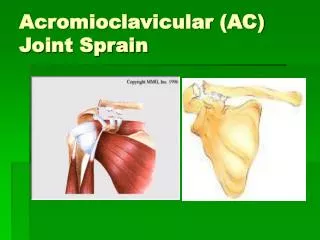
AC Joint • Diarthrodial joint between medial facet of acromion and the lateral (distal) clavicle. • Contains intra-articular disk of variable size. • Thin capsule stabilized by ligaments on all sides: • AC ligaments control horizontal (anteroposterior ) displacement • Superior AC ligament most important
Distal Clavicle • Coracoclavicular ligaments • “Suspensory ligaments of the upper extremity” • Two components: • Trapezoid • Conoid • Stronger than AC ligaments • Provide vertical stability to AC joint
Mechanism of Injury Moderate or high-energy traumatic impacts to the shoulder • Fall from height • Motor vehicle accident • Sports injury • Blow to the point of the shoulder • Rarely a direct injury to the clavicle
Physical Examination • Inspection • Evaluate deformity and/or displacement • Beware of rare inferior or posterior displacement of distal or medial ends of clavicle • Compare to opposite side.
Physical Examination • Palpation • Evaluate pain • Look for instability with stress
Physical Examination • Neurovascular examination • Evaluate upper extremity motor and sensation • Measure shoulder range-of-motion
Radiographic Evaluationof the Clavicle • Anteroposterior View • 30-degree Cephalic Tilt View
Radiographic Evaluation of the Clavicle • Quesana View • 45-degree angle superiorly and a 45-degree angle inferiorly • Provide better assessment of the extent of displacement
Radiographic Evaluationof the AC Joint • Zanca View • AP view centered at AC joint with 10 degree cephalic tilt • Less voltage than used for AP shoulder
Stress Views of the Distal Clavicle & AC Joint • Rationale: will demonstrate instability and differentiate grade III AC separations from partial Grade I-II injuries • Performed by having patient hold 10# weight with injured arm • Rarely used today, since most AC joint injuries treated the same, and management of distal clavicle fractures depends on initial displacement and location of fracture.
Radiographic Evaluation of the Medial One Third • X-ray: Cephalic tilt view of 40 to 45 degrees • CT scan usually indicated to best assess degree and direction of displacement
Classification ofClavicle Fractures • Group I : Middle third • Most common (80% of clavicle fractures) • Group II: Distal third • 10-15% of clavicle injuries • Group III: Medial third • Least common (approx. 5%)
Treatment Options • Nonoperative • Sling • Brace • Surgical • Plate Fixation • Screw or Pin Fixation
Nonoperative Treatment • “Standard of Care” for most clavicle fractures. • Continued questions about the need to wear a specialized brace.
Simple Sling vs.Figure-of-8 Bandage • Prospective randomized trial of 61 patients • Simple sling • Less discomfort • Functional and cosmetic results identical • Alignment of healed fractures unchanged from the initial displacement in both groups Andersen et al., Acta Orthop Scand 58: 71-4, 1987.
Nonoperative Treatment • It is difficult to reduce clavicle fractures by closed means. • Most clavicle fractures unite rapidly despite displacement • Significantly displaced mid-shaft and distal-third injuries have a higher incidence of nonunion.
Nonoperative Treatment • There is new evidence that the outcome of nonoperative management of displaced middle-third clavicle fractures is not as good as traditionally thought, with many patients having significant functional problems.
Deficits following nonoperative treatment of displaced midshaft clavicular fractures • A patient-based outcome questionnaire and muscle-strength testing were used to evaluate 30 patients after nonoperative care of a displaced midshaft fracture of the clavicle. • At a minimum of twelve months (mean 55 mos), outcomes were measured with the Constant shoulder score and the DASH patient questionnaire. In addition, shoulder muscle-strength testing was performed with the Baltimore Therapeutic Equipment Work Simulator, with the uninjured arm serving as a control. McKee et al. J Bone Joint Surg Am 2006;88-A:35-40.
Deficits following nonoperative treatment of displaced midshaft clavicular fractures • The strength of the injured shoulder was 81% for maximum flexion, 75% for endurance of flexion, 82% for maximum abduction, 67% for endurance of abduction, 81% for maximum external rotation, 82% for endurance of external rotation, 85% for maximum internal rotation, and 78% for endurance of internal rotation (p < 0.05 for all). • The mean Constant score was 71 points, and the mean DASH score was 24.6 points, indicating substantial residual disability. McKee et al. J Bone Joint Surg Am 2006;88-A:35-40.
Displaced midshaft clavicle fractures can cause significant, persistent disability, even if they heal uneventfully.
Definite Indications for Surgical Treatment of Clavicle Fractures • 1) Open fractures • 2) Associated neurovascular injury
Relative Indications for Acute Treatment of Clavicle Fractures • 1) Widely displaced fractures • 2) Multiple trauma • 3) Displaced distal-third fractures
Relative Indications for Acute Treatment of Clavicle Fractures • 4) Floating shoulder • 5) Seizure disorder • 6) Cosmetic deformity • 7) Earlier return to work.
Clavicular Displacement • < 5 mm shortening: acceptable results at 5 years (Nordqvist et al, Acta Orthop Scand 1997;68:349-51. • > 20 mm shortening associated with increased risk of nonunion and poor functional outcome at 3 years (Hill et al, JBJS 1997;79B: 537-9)
Plate Fixation • Traditional means of ORIF • Plate applied superiorly or inferiorly • Inferior plating associated with lower risk of hardware prominence • Used for acute displaced fractures and nonunions.
Intramedullary Fixation • Large threaded cannulated screws • Flexible elastic nails • K-wires • Associated with risk of migration • Useful when plate fixation contra-indicated • Bad skin • Severe osteopenia • Fixation less secure
Complications of Clavicular Fractures and its Treatment • Nonunion • Malunion • Neurovascular Sequelae • Post-Traumatic Arthritis
Risk Factors for the Development of Clavicular Nonunions • Location of Fracture • (outer third) • Degree of Displacement • (marked displacement) • Primary Open Reduction
Principles for the Treatment of Clavicular Nonunions • Restore length of clavicle • May need intercalary bone graft • Rigid internal fixation, usually with a plate • Iliac crest bone graft • Role of bone-graft substitutes not yet defined.
Clavicular Malunion • Symptoms of pain, fatigue, cosmetic deformity. • Initially treat with strengthening, especially of scapulothoracic stabilizers. • Consider osteotomy, internal fixation in rare cases in which nonoperative treatment fails. Correction of malunion with thoracic outlet sx
Neurologic Sequelae • Occasionally, fracture fragments or abundant callus can cause brachial plexus symptoms. • Treatment is reduction and fixation of the fracture, or resection of callus with or without osteotomy and fixation for malunions.
Osteotomy for Clavicular Malunion • 15 patients with malunion after nonoperative treatment of a displaced midshaft clavicle fracture of the clavicle. Average clavicular shortening was 2.9 cm (range, 1.6 to 4.0 cm). • Mean time from the injury to presentation was three years (range, 1 to 15 years). • Outcome scores revealed major functional deficits. • All patients underwent corrective osteotomy of the malunion through the original fracture line and internal fixation. McKee MD, et al. J Bone Joint Surg Am 2003;85-A(5):790-7
Osteotomy forClavicular Malunion • At follow-up (mean 20 months postoperatively) the osteotomy site had united in 14 of 15 patients. • All 14 patients satisfied with the result. • Mean DASH score for all 15 patients improved from 32 points preoperatively to 12 points at the time of follow-up (p = 0.001). • Mean shortening of the clavicle improved from 2.9 to 0.4 cm (p = 0.01). • There was 1 nonunion, and 2 patients had elective removal of the plate. McKee MD, et al. J Bone Joint Surg Am 2003;85-A(5):790-7
Classification of Distal Clavicular Fractures(Group II Clavicle Fractures) • Type I-nondisplaced • Between the CC and AC ligaments with ligament still intact From Nuber GW and Bowen MK, JAAOS, 5:11, 1997
Classification of Distal Clavicular Fractures • Type II • Typically displaced secondary to a fracture medial to the coracoclavicular ligaments, keeping the distal fragment reduced while allowing the medial fragmetn to displace superiorly • Highest rate of nonunion (up to 30%) • Two Types