Download

1 / 32
490 likes | 3.55k Views
Sternoclavicular joint dislocation. Jason Blackham, MD Clinical Assistant Professor Division of General Internal Medicine University of Iowa Sports Medicine Center. History. 17 yo high school quarterback was sacked during a game Complained of Right antero-inferior neck pain Dyspnea

E N D
Sternoclavicular joint dislocation Jason Blackham, MD Clinical Assistant Professor Division of General InternalMedicine University of Iowa Sports Medicine Center
History • 17 yo high school quarterback was sacked during a game • Complained of • Right antero-inferior neck pain • Dyspnea • Dysphagia • Unremarkable PMH
Physical Exam • RR 20, HR 84 • Normal mentation and no resp distress • Neurological exam normal • Pain with palpation of right clavicle • Loss of fullness of proximal clavicle • No skin tenting
Physical Exam • Walked off the field • Postured with head tilted (R), arm at side in IR with elbow at 90 degrees flexion • Off field exam • Trachea midline, no stridor • Breath sounds normal, symmetric, resonant • No cardiac murmer or rub and symmetric pulses • Transported to ED
Differential Diagnosis • Shoulder dislocation • Proximal clavicular fracture • Sternoclavicular joint dislocation • Traumatic pneumothorax
AF C C BV T BV E BA R
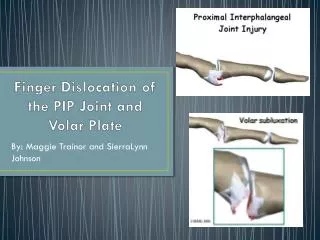
Diagnosis • Posterior sternoclavicular joint dislocation with avulsion fracture
Treatment • Reduction under general anesthesia • 4 weeks immobilized in sling • 2 weeks of protected ROM, strengthening • Cornerback for 3 weeks • Returned to quarterback at 9 weeks
40% MVC 21% Sports 39% Other Trauma ~3% of all shoulder girdle injuries > 90% anterior dislocations Epidemiology Clin Sports Med 2003;22:387-405 Phys Sports Med 1999;27(2):105-13
Mechanisms of Posterior • Fall on shoulder with arm flexed and adducted • Lateral force to shoulder when shoulder rolled forward • Posterolateral force to shoulder while opposite shoulder on ground • Force to anteromedial clavicle Clin Sports Med 2003;22:387-405 Military Med 2004;169(2):134-6 Rockwood and Green’s Fractures in Adults. 1997
Complications of Anterior • SC joint arthritis • Cosmetic appearance • Persistent prominence • Chronic pain • Recurrent instability
Complications of Posterior • Pneumothorax • Compression or laceration • Trachea • Esophagus • Artery / Vein • SVC laceration • Brachial plexus injury • Thoracic outlet obstruction J Trauma 1998;44(2):381-3 Clin Sports Med 2003;22:371-85
Treatment of Anterior • Anterior Dislocation • Controversial • Majority unstable following reduction • Sling immobilization for 6 weeks • If continued symptoms, surgery
Treatment of Posterior • Recommendation is for closed reduction • <48 hrs to <7 days of injury • Sling or figure-of-eight • Single review article & case studies • good results • If unstable or complications, then open Clin Sports Med 2003;22:359-70 Clin Sports Med 2003;22:387-405 Can J Surgery 1986;29(2):104-6 J Trauma 1967;7(3):416-23
Return to Play • Sling or figure-eight harness for 4-6 weeks • Return when pain free motion • may require additional 4-8 weeks Military Med 2004;169(2):134-6 Phys Sports Med 1999;27(2):105-13
Operative Treatment • Claviculectomy • Resection of medial clavicle • Reconstruction of capsule or ligaments • Not pinning • Migration of transfixion pins
Operative Treatment • Capsule repair with tendon graft • Burrow’s procedure • Sublcavius tendon tenodesis • Fascia lata graft • Sternocleidomastoid muscle • Medial clavicle osteotomy
Outcome • Completed FB season without pain or instability • Pitched for high school baseball team
Summary • Posterior SC dislocations are rare • Potentially severe complications • Closed reduction is preferred • RTP after healing and ROM regained • generally 6-14 weeks