Download
1 / 41
430 likes | 571 Views
SWEAT TEST. Doç. Dr. Deniz DOĞRU ERSÖZ Hacettepe University Faculty of Medicine Pediatric Pulmonary Medicine Unit. DIAGNOSIS OF CYSTIC FIBROSIS. One or more characteristic phenotypıc feature or a history of a sibling with CF or a positive newborn screening test result. and.

E N D
SWEAT TEST Doç. Dr. Deniz DOĞRU ERSÖZ Hacettepe University Faculty of Medicine Pediatric Pulmonary Medicine Unit
DIAGNOSIS OF CYSTIC FIBROSIS One or more characteristic phenotypıc feature or a history of a sibling with CF or a positive newborn screening test result and Two or more high sweat chloride test or two CF mutations or abnormal nasal potential difference test Rosenstein BJ, Cutting GR. The diagnosis of cystic fibrosis: a consensus statement. Cystic Fibrosis Foundation Consensus Panel. J Pediatr 1998;132:589-95.
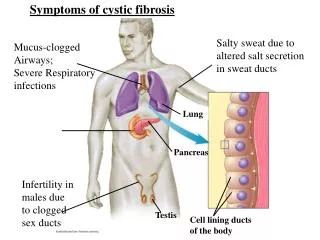
Sweat Test • In CF, there are high concentrations of chloride and sodium in sweat because of abnormal ion transport • Sweat test is the “gold standard” for diagnosis of CF • 98% of CF patients have elevated chloride in sweat
Sweat Test • Sodium or chloride can be measured • Chloride provides more accuracy than sodium • Both are increased in CF • In CF Na/Cl<1
Sweat Test Methodology • Sweat collection • Sweat analysis • Quantitative pilocarpine ionthophoresis test(Gibson Cooke test) • Conductivity • Osmolarity
Sweat collection • Chemical pilocarpine is applied to a small area on an arm or leg • A copper electrode is attached and a weak electrical current is applied to stimulate sweating (5 mV in 5-10 minutes)
Sweat collection 3. The sweat is collected onto gauze, filter paper (Gibson Cooke) capillary tube (Macroduct)
Sweat collection • The sweat is collected during a 30-min period. • The collected sample is sent to a laboratory for • quantitative analysis of chloride • conductivity • osmolarity • 6. Sweat should not be stimulated from head, trunk, or any area of inflammation or serous or bloody discharge
Sweat Test Methodology • Sweat collection • Sweat analysis • Quantitative pilocarpine ionthophoresis test(Gibson Cooke test) • Conductivity • Osmolarity
Quantitative pilocarpine iontophoresis test(Gibson Cooke test)
Quantitative pilocarpine iontophoresis test (Gibson Cooke test) • The most discriminatory test for diagnosis • Quantitative analysis of sweat chloride level • The reference values for sweatchloride are: • less than 40 mmol/l: negative • 40–60 mmol/l: borderline • greater than 60 mmol/l: CF
Quantitative pilocarpine iontophoresis test (Gibson Cooke test) Sweat chloride concentration greater than 160 mmol/l is not physiologically possible and indicates that there is an error
Quantitative pilocarpine iontophoresis test (Gibson Cooke test) • Newborns • During the first 24 hours after birth, sweat electrolytes may be transiently elevated in normal infants • After the first 2 days, there is a rapid decline • Sweat tests should be obtained when the child is at least 48 hours old
Quantitative pilocarpine iontophoresis test (Gibson Cooke test) • Newborns • Normal newborns typically have very low • concentrationsof sweat chloride (less than 10 mmol/L) • A value of 30−40 mmol/l is highlysuspicious for CF
Sweat Test Methodology • Sweat collection • Sweat analysis • Quantitative pilocarpine ionthophoresis test(Gibson Cooke test) • Conductivity • Osmolarity
Conductivity • Indirect physical chemical measurement • Provides approximationsof electrolyte levels in sweat • Approved for screening only • Measures other unmeasured charged species insweat, including lactate, bicarbonate, sodium, potassiumand chloride • Conductivity is approximately15 mmol/l higher than sweat chloride alone
Conductivity A patient with a positiveor borderline result from conductivity test should be referredto a testing center for a pilocarpine iontophoresisstimulated direct measurement of sweat electrolytes forconfirmation
Conductivity High levels of false-positive and false-negative results
Conductivity • Wescor Sweat-Chek conductivityanalyzer (Wescor, • Logan,UT) • Orion skinelectrode for chloride (Orion Research, • Cambridge, MA) • Scandipharm CF Indicator System chloride patch • (Scandipharm, Birmingham, AL)
Quantitative pilocarpine Conductivity iontophoresis test Normal 0-40 mmol/l 0-60 mmol/l Borderline 40-60 mmol/l 60-90 mmol/l Positive 60 mmol/l and more 90 mmol/l and more
Macroduct conductivitysystem • Advantages • Undiluted sweat • samples • Small amounts of sweat (10–15 μl) • Use liquid collecteddirectly from the iontophoresis area • Disadvantages • Need for atrained staff • Frequent calibration • and cleaning of the instrument • Cost
Sweat chloride values • may vary depending on • Method of sweat stimulation • Weight of the sweat sample • Sweat secretory rate • Salt intake • Nutritional status • Hidration status
Errors in Sweat Test • False positive rate: %15 • False negative rate: % 12
Errors in Sweat Test • Unreliable methodology • Inadequate sweat collection • Tecnical errors • Misinterpretation of results
Tecnical Errors in Sweat Test • Skin contamination by salt containing materials • Failure to dry the patient’s skin before sweat collection • Evaporation of sweat sample during collection and transport • Errors in sample weighing, dilution, electrolyte analysis • Continuing sweat collection after 30 minutes
Interpretation Errors in Sweat Test • Using chloride analyte reference values for conductivity measurements • Quantitative pilocarpine Conductivity • iontophoresis test • Normal 0-40 mmol/l 0-60 mmol/l • Borderline 40-60 mmol/l 60-90 mmol/l • Positive 60 mmol/l and more 90 mmol/l and more
Interpretation Errors in Sweat Test • Establishement of a diagnosis of CF on the basis of a single positive test • Failure to repeat a test giving borderline results • Failure to repeat a test in a patient with a negative result but a clinical picture highly suggestive of CF
Conditions other than CF associated with an elevated sweat chloride Adrenal insufficiency Anorexia nervosa Atopic dermatitis Exercise Familial hypoparathyroidism Malnutrition Nephrojenik diabetes insipidus Nephrosis Long term prostoglandin E1 infusion Protein calorie malnutrition Pseudohypoaldosteronizm Psychosocialfailure to thrive Autonomic disfunction Celiac disease Ectodermal dysplasia Familial cholestasis Fucosidosis Glucose-6-phosphate dehydrogenase deficiency Hypogammaglobulinemia Kleinfelter Syndrome Mauriac Syndrome Mucopolysaccaridosis Type 1 Reverts to normal with resolution of underlying condition
False negative sweat test results • Tecnical errors • Inadequate volume of sweat • Edema
CFTR Mutations Associated WithBorderline or Normal Sweat Chloride Levels 3849+10 kb C>T R117H G551S A455E D1152H IVS8 (5T) L206W 2789+5 G>A
Indications for Repeat Sweat Testing • All positive sweat tests • All borderline sweat tests • Patients thought to have CF who do not follow an expected clinical course
Indications for Repeat Sweat Testing • Repeat testing should be carried • when the patient is • clinically stable • well hydrated • free of acute infection • not receiving mineralocorticoids
CF unlikely Negative Sweat test X2 Positive CF confirmed Borderline Nasal PD CF confirmed CF ruled out Abnormal Normal Not available CF confirmed One CF allele 2 CF alleles DNA analysis CF or carrier No CF allele Sputum, throat or BAL cultures Sputum, throat or BAL cultures
Sputum, throat or BAL cultures P. aeruginosa CF likely No P. aeruginosa Evaluate pancreatic function Sinus X- ray Semen analysis Sperm present Sperm absent Normal Abnormal Clear Pansinusitis CF more likely CF unikely CF less likely CF more likely CF unikely
A recent national audit showed widely variablepractice and standards in sweat testing: • a lack of sweat chlorideanalysis by some laboratories • variability inreference ranges • lack of quality control • sporadic reports of adverse events The SpecialistAdvisory Group for Paediatric Investigations ofthe UK National E External Quality AssuranceSchemes (NEQAS) suggested that an evidencebased guideline
Key points from the guideline Explain the test adequatelybeforehand, supported by a writteninformation sheet (grade C) Sweat tests can be performed after 2 weeks ofage in infantsgreater than 3 kg who arenormally hydrated and without significantsystemic illness (grade C) Sweat tests should be delayed in subjects whoare oedematous or on systemic steroids (gradeC) For safety reasons sweat tests should not beperformed in subjects who are on oxygen byan open delivery system(grade C)
Key points from the guideline The stimulation, collection, storage, and analysisof sweat must be performed according towritten standard operating proceduresconsistentwith the recommendations in theguideline (grades B or C). Sweat should be collected for not more than30 minutes and not less than 20 minutes(grade B) Non-standard or hybrid methods for sweatstimulation and collection should not be used(grade B). Centres should only analyse sweat if theyundertake a minimum number of 50 tests perannum (grade C), with a minimum of 10collection procedures undertaken per person(grade C). Sweat collection must be performed by fullytrained personnel(grade C).
Key points from the guideline The sweat test report should include the sweat weight/volume collected (grade C) Sweat chloride is the best discriminator and must alwaysbe included (grade B) Sweat conductivity requires further research before it canbe relied on for diagnosis (grade B) Sweat sodium should not be interpreted without achloride result. Sweat potassium and osmolality are notrecommended (grade B)
Risks Associatedwith Sweat Testing • Urticaria or burn • reaction to pilocarpine orelectrical stimulation • iontophoresis current greater than 4 mA • skincoming into contact with the bare metal of the electrode • reagent interface not being moist enough • damaged electrode surface • Theserisks rarely manifest with properly trained technicians
Conclusion • An accurate sweat-test relies on the exact coordinationof • manyelements • Tests must be performed by competent personnel andproper use of equipment • Centers performing sweat-tests should follow agreed-upon • guidelines • Sweat-testing should be restricted to centers that perform • a significant amount of tests yearly