Download
1 / 26
260 likes | 503 Views
Sexually Transmitted Diseases(STDs):. -STDs are well-defined group of infectious diseases with the highest frequency in USA (as reported by CDC ). -STDs were ranked among the most important infectious diseases with regard to the physical, psychological, and

E N D
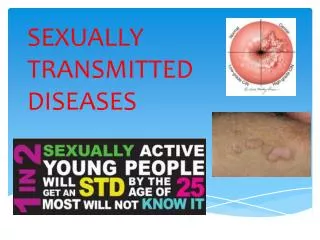
Sexually Transmitted Diseases(STDs): -STDs are well-defined group of infectious diseases with the highest frequency in USA (as reported by CDC). -STDs were ranked among the most important infectious diseases with regard to the physical, psychological, and economic damage they cause to humans. -Highly varied microbial classes could cause different types of STDs.
Epidemiology: Worldwide, nearly a million people acquire an STD, including the HIV, every day, with the highest frequency among marginalized population who have difficulty accessing health care services. Currently, more than 30 diseases are known to spread through sexual activity; -Chlamydial infection. -Gonorrhea -Genital herpes. -Trichomoniasis. -Warts. -AIDS. -Syphilis. -Chancroid. -Candidiasis. -Bacterial vaginosis.
STDs Entry, spread, damage, and complications: -Most of the STD-causing agents enter the body at local sites, through the mucosal or squamous epithelial layers of the urethra, cervix, rectum, or vagina. Damage: The acute manifestations of the most frequent STDs are classified into two groups: 1-Mucopurulent Urethritis and Cervicitis: Example: Gonorrhea and Chlamydial infection. 2-Genital Ulcer disease: Example: Syphilis, Chancroid, and Genital herpes.
N -STDs Reservoir: Asymptomatic human carriers. -Spread: Each agent has a different escape mechanism. -The most serious consequences of STDs include: (Most complications experienced by Women): 1-Pelvicinflammatorydisease (PID). 2-Anogenital or Cervical cancer. 3-Infertility or spontaneous abortion. 4-Congenital and neonatal infections. 4-Premature delivery or ectopic pregnancy. 5-Secondary and tertiary syphilis. 6-Recurrent herpes infection.
Gonorrhea:Neisseria gonorrhoeaeinfection: Gonorrhea is a specific type of urethritisthat practically always involves mucousmembranes, and epithelial layersof the urethra, resulting in a copious -purulent discharge of pus. - CDCestimates that more than 700,000 people in the United States get new gonorrheal infections each year. -African Americans are the most affected group (69% in 2010). -WHOestimates that 62 million cases of gonorrhea appear each year.
Pathogenesis and tissue damage: -Humans are the only reservoir. -Asymptomatic carriage is greater among women. -Adolescent female has larger zone of ectopy for columnar epithelial cells (in the Ectocervix). -Attachmentof microbe via its pilito the non-ciliated columnar epithelialcells of male urethra and female Endocervix.
N -Microbial multiplication and inflammation due to: 1-IgA Protease: Escape humoral response. 2-Phase variation: Turning on /off genes of surface adherence components: Escape neutrophil killing. 3-The microbial lipooligosaccharide: Polyclonal B lymphocyte activator. Death of ciliated-epithelial cells: TNF-α production. -Urethritisand Cervicitis.
N -Exogenous Neisseria gonorrhoeae, other pathogens, and Endogenous vaginal flora will ascend to female upper reproductive tract due to: A-Loss of Endocervix mucus production . B-End of Menses (Menstrual cycle; loss of mucus). The ascending infection results in Pelvic inflammatory disease (PID): 1-Endometritis: Endometrium infection (Columnar epith.) 2-Salpingitis : Fallopian tubes infection. 3-Ovaritis. -DGI: Septic arthritis and Tenosynovitis.
N -N. gonorrhoeae infectionin adolescent female causes Vulvovaginitis. Other causative agents of Pelvic inflammatory disease: 1-Chlamydiatrachomatis. 2-Mycoplasmahominis. 3-Mycoplasmagenitalium. 4-Ureaplasmaurealyticum 5-Endogenous E. coli. -60% of cases are subclinical with no or mild symptoms. -Late complications: infertility, ectopic pregnancy, chronic pelvic pain.
N Neisseria gonorrhoeae infectionin male: -Urethritis: Dysuria, redness, and Painful thick copious-( greenish- yellow) discharge of pus. -The infection could be disseminated tothe epididymis (epididymitis), prostate gland (prostatitis), testicular tissue (orchitis).
N Systemic dissemination of gonorrhea resulting in skinpustules, septic arthritis, bacteremia (rare), and endocarditis (rare).
Diagnosis of Neisseria gonorrhoeae infection: Clinical specimens: Urethral discharge, vaginal discharge. Direct detection: 1-Microscopic examination of Gram’s stained smear: Intracellular Gram-negative diplococci present in the polymorphonuclear leukocytes.
N 2-Culture: -Neisseria gonorrhoeae species are fastidious bacteria: 1-NADPandHemoglobin (X and V factor): So the bacteria grow best on Chocolate agar. 2-A 5-10% CO2 for primary isolation. -All species are oxidase positive. -Selective medium: Thayer-Martin agar: contains antibiotics ( Vancomycin, Colistin, and Nystatin).
N 3-PCR: Detection of microbial genetic material in the clinical specimen. 4-Antibiotic sensitivity test: -More than 20% of current isolates are resistant to penicillin due to Beta-Lactamase plasmids. -Penicillinase-producing N. gonorrhoeae (PPNG) strains are sensitive to Third generation Cephalosporin.
Syphilis:Treponema pallidium infection: -Syphilis is a sexually transmitted disease caused by the spirochete Treponema pallidium. -The microbe could be transmitted to fetus from infected mother (Transplacentation route, Congenital syphilis) after the first ten to fifteen weeks of pregnancy. -Congenital syphilis is associated with: 1-Intrauterine growth retardation. 2-Hepatosplenomegaly, CNS infection, and mucocutaneous lesions, and lymphadenopathy.
Pathogenesis and tissue damage: Primary syphilis: -The bacterium enters the body through a break in the skin, or by penetratingmucous membranes of the genitalia. -After the average period of three weeks of inoculation, the Syphilitic Chancre appears as a first manifestation of the disease. -A chancre is a single, painless, non-itchy skin ulceration with a clean base and sharp borders between 0.3 and 3.0 cm in size.
N Tissue destruction in primary syphilis is induced by: 1-The microbial virulence: The microbial Hyaluronidase destroy the polysaccharide (hyaluronic acid; glycosaminoglycan) that holds host cells together in the extracellular matrix. 2-The Cellular immune defenses: (Neutrophils, lymphocytes, and macrophage). against replicating Treponema and tissue.
N -The primary lesion heals spontaneously, but the microbe continues to spread throughout the body via the lymph and blood in asymptomatic period lasting as long as 24 weeks. Secondary Syphilis: -It is characterized by appearance of a red -maculopapularrash on almost any part of the body. -In the anogenital region: Condylomata lata. -Hepatitis, Glomerulonephritis, and meningitis.
N -A macule is a change in surface color, without elevation or depression. -A papule is a circular, solid elevation of skin with no visible fluid, varying in size from a pinhead to less than 5 to 10 mm in diameter.
N Latent Syphilis stage : -After healing of secondary syphilis, the microbe enters a latency period that can last 3 to 30 years. - This stage shown in two-thirds of individuals who acquired primary syphilis. - In one-half of this group, tertiary syphilis is established. In this period (Latent syphilis): 1-No primary or secondary symptoms (asymptomatic period). 2- Serologic tests show positive results.
N Tertiary syphilis: Tertiary syphilis may occur approximately three to 15 years after the initial infection. It is divided into three different forms: A-Gummatous syphilis : ( granulomatous lesions of liver, skin, and bones (15%). B-Neurosyphilis (6.5%): infection of Brain parenchyma, dorsal column of spinal cord. C-Cardiovascularsyphilis (10%): Vasculitis and aortic valve insufficiency.
Diagnosis of Syphilis: Clinical specimens: Exudate (pus), tissue biopsy, and serum specimens. Direct: In Microbiology Lab: A- Darkfield Microscopy: Rotary Corkscrew-like motility with 90 ˚ angulation. B- Immunofluorescent microscopy: staining of microbe by Anti-Treponema antibodies. In Histology Lab: Bright-field Microscopy: modified Steiner silver stain.
N Cultivation of Treponema pallidium: -The microbe is extremely fastidious(small genetic material), and fragile; sensitive to disinfectant, heat, and drying. -Treponema pallidum is a chemoheterotrophic, secretes the enzyme hyaluronidase. -The bacterium does not grow in conventional culture media. -Animal inoculation could be used for cultivation of microbe in vivo: -All species are sensitive to penicillin. -Alternate therapy: Tetracycline and Erythromycin.
N Indirect diagnosis: In Serology: A-Nontreponemaltest (non-specific): Anti-Cardiolipinantibodies by VDRL or RPR test. B- Treponemal test (specific): Detection of anti-treponema antibodies by TPHAor IFA.