Download
1 / 31
320 likes | 527 Views
New Antibiotics for Old Problems. David A. Pegues, M.D. Division of Infectious Diseases David Geffen School of Medicine at UCLA. Vancomycin for MRSA pneumonia: is it obsolete?. Pneumonia (%). Most Common Isolates: All ICU HAP vs VAP. 20. 18. 18. 18. 18. 17. 16. All HAP. *. 14.

E N D
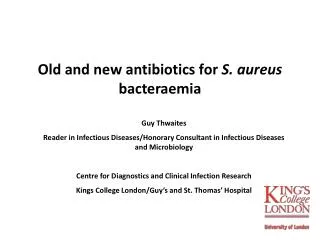
New Antibiotics for Old Problems David A. Pegues, M.D. Division of Infectious Diseases David Geffen School of Medicine at UCLA
Vancomycin for MRSA pneumonia: is it obsolete?
Pneumonia (%) Most Common Isolates: All ICU HAP vs VAP 20 18 18 18 18 17 16 All HAP * 14 VAP † 12 12 11 10 8 7 7 6 5 5 4 4 4 4 4 2 0 S aureus Pseudomonas Enterobacter spp Klebsiella Candida albicans Escherichia coli Haemophilus aeruginosa pneumoniae influenzae *January 1992-May 1999. †1990-1995. NNIS. Am J Infect Control. 1999;27:520-532. Fridkin SK et al. Infect Dis Clin North Am. 1997;11:479-496.
Vancomycin • “Gold standard” of therapy for MRSA • Poor concentration in lung and CSF • Nephrotoxicity ~1.4%, ototoxicity uncommon • Emerging concerns: • VRSA, VISA • heteroresistant strains • vancomycin MIC creep1 • UCLA 2004--MIC = 1 (70.4%) or 2 ( 0.4%) • agr mutations 1 Wang G, et al. J Clin Microbiol 2006;44:3883-6.
Drug Concentration in epithelial Lining Fluid Drug at 4 hrs Stevens DL. Clin Infect Dis 2006;42:S51.
Vancomycin PK and Treatment of MRSA HCAP • 102 patients BAL+ MRSA HCAP • Examined vancomycin PK and correlated PK with mortality • Neither Trough >15 mcg/ml or AUC >400 mcg hr/ml were associated with survival benefit Jeffres MN, et al. Chest 2006 130:947.
Vancomycin Nephrotoxicity 25% reduction in GFR Jeffres MN, et al. ClinTher 2007
High-Dose Vancomycin Therapy for MRSA Infections: Efficacy and Toxicity Initial response (72 hrs) Final response (end of Rx) Hidayat LK, et al. Arch Intern Med 2006;166:2138-44.
Linezolid vs Vancomycin in VAP by MRSA Linezolid Vancomycin 100 90 80 84.1 70 60 Clinical cure (% of patients) 62.2 61.7 60.5 50 53.7 37.7 48.9 36.7 35.2 40 45.4 30 20 22.9 21.2 10 P= 0.07 P= 0.02 P= 0.06 P= 0.02 P= 0001 P= 0.001 0 VAP Gram+ VAP S. aureus MRSA VAP Survival Eradication VAP (N=434) (N=214) (N=179) (N=70) Kollef MH, et al. Intensive Care Med 2004;30:388-94.
Linezolid vs. Vancomycin for VAP • Linezolid is an alternative to vancomycin for the treatment of MRSA VAP and may be preferred on the basis of a subset analysis of two prospective randomized trials (Level II) • Linezolid may also be preferred if patients have renal insufficiency or are receiving other nephrotoxic agents, but more data are needed (Level III). Niederman MS, et al. Am J Respir Crit Care Med. 2005;171:402.
MetronidazoleforClostridiumdifficile associateddisease:isit okayformom?
Increasing Severity and Costs of CDAD • Boston, 19981 • Very low attributable mortality • Average of $3,600 excess costs per case • Average of 3.6 extra hospital days • Pittsburgh, 20002 • Life-threatening disease from 1.6% to 3.2% • 44 colectomies and 20 deaths 1 Kyne L, et al. Clin Infect Dis. 2002;34:346-353. 2 Dallal RM, et al. Ann Surg. 2002;235:363-372.
Toxin production by an emerging strain of C. difficile associated with outbreaks of severe disease Growth Curve Toxin Production Warny M, et al. Lancet 2005:366:1079.
Studies of Metronidazole Treatment in CDAD: Treatment Failure and Recurrences StudiesRx failures Recurrences F/U (d) F+R (%) Cherry et al, 1982 0/13 2/13 (15%) 30 15% Teasley et al, 1983 2/42 (5%) 2/39 (5%) 21 10% Olson et al, 1994 14/632 (2%) 39/632 (6%) 30 8% Wenisch et al, 1996 2/31 (6%) 5/31 (16%) 30 22% Kyne et al, 2001 .. 22/44 (50%) 60 .. Fernandez et al, 2004 38/99 (38%) .. .. .. Musher et al, 2005 46/207 (22%) 58/207 (28%) 90 50% Pepin et al, 2005178/1123 (16%) 243/845 (29%) 60 45% Aslam D, et al. Lancet Infect Dis 2005;5:549-57.
Studies of Vancomycin Treatment in CDAD: Treatment Failure and Recurrences StudiesRx failures Recurrences F/U (d) F+R (%) Bartlett et al, 1980 3/79 (4%) 11/79 (14%) 30 18% Silva et al, 1981 0/16 2/16 (13%) 42 13% Teasley et al, 1983 0/52 6/51 (12%) 21 12% Bartlett, 1984 6/189 (3%) 46/189 (24%) 25 27% Young et al, 1985 8/42 (19%) 11/30 (37%) 30 56% Dudley et al, 1986 0/15 3/15 (20%) 60 20% de Lalla et al, 1989 2/25 (8%) 3/25 (12%) 30 20% Fekety et al, 1989 0/46 9/46 (20%) 42 20% de Lalla et al, 1992 0/20 4/20 (20%) 30 20% Olson et al, 1994 1/122 (1%) 12/122 (10%) 30 11% Wenisch et al, 1996 2/31 (6%) 5/31 (16%) 30 22% Pepin et al, 2005 .. 31/112 (28%) 60 .. Aslam D, et al. Lancet Infect Dis 2005;5:549-57.
Other Therapies for CDAD • Bacitracin • Teicoplanin and fusidic acid • Nitazoxanide • blocks anaerobic metabolic pathways • MIC90 0.06–0.5 μg/mL • Open-label study: cured 75% of patients who had failed metronidazole therapy;1/3 relapsed • Rifampin, rifaximin
Diseaseseverity No. of patients cured/no. of patients treated (%) P Mtz group Vm group Total Mild 37/41 (90) 39/40 (98) 76/81 (94) .36 Severe 29/38 (76) 30/31 (97) 59/69 (86) .02 All 66/79 (84) 69/71 (97) 135/150 (90) Vancomycin vs. Metronidazole for the Treatment of CDAD • Methods: Oct. 1994– Jun. 2002, patientswith CDAD stratified as having mild or severedisease based on clinicalcriteria • Intervention: oralmetronidazole (250 mg 4times per day) ororal vancomycin (125 mg4 times per day)for 10 days Zar FA, et al. Clin Infect Dis 2007;45:302-7.
Patient Characteristics and Response to Metronidazole (MTZ) Zar FA, et al. Clin Infect Dis 2007;45:302-7.
Species Distribution and Crude Mortality for 1890 Cases of Candida BSI, 1995-2002 Wisplinghoff H, et al. Clin Infect Dis 2003;36:1103-10
Spectrum of Activity: Echinocandins Activity Species Highly Active Low MIC, with fungicidal activity and good in-vivo activity C. albicans C. glabrata C. tropicalis C. krusei C. kefyr P. jiroveci Very Active Low MIC, but without fungicidal activity in most instances C. parapsilosisC. gulliermondiiC. lusitaniae A. fumigatusA. flavusA. terreus Some Activity Detectable activity, which might have therapeutic potential for man (in some cases in combination with other drugs). C. immitisB. dermatididisScedosporium spp P. variotiiH. capsulatum Inactive No intrisic activity Zygomycetes Cryptococcus neoformans Fusarium spp Trichosporon spp Denning DW, Lancet 2003 (Oct 4);1142-51.
Anidulafungin versus Fluconazole for Invasive Candidiasis • Design: DB, R, MC non-inferiority trial comparing: • Anidulafungin 200 mg once then 100 mg QD x 14 days • Fluconazole 800 mg once then 400 mg QD x 14 days • Could switch to fluconazole 400 mg PO QD after 10 days • Setting: 33 sites in US, 8 in Canada, 6 in Europe • Patients: 261 enrolled, 245 in MITT analysis • Results: • Candida albicans--62% of episodes; in vitro FLU resistance uncommon • Treatment success at end of IV therapy: 75.6% ANF vs. 60.2% FLU • All cause death rate: 23% ANF vs. 31% FLU (P=0.13) • Conclusion: Anidulafungin was noninferior to fluconazolein the treatment of invasive candidiasis Reboli AC, et al. N Engl J Med 2007; 356:2472-82.
Baseline Patient Characteristics Reboli AC, et al. N Engl J Med 2007; 356:2472-82.
Global Response to Treatment for MITT Population Reboli AC, et al. N Engl J Med 2007; 356:2472-82.
Risk of Hospital Mortality and Timing of Antifungal Therapy for Candidemia • Retrospective cohort analysis • 151 episodes of Candidemia over 4-yr period; BJH • 50 (31.8%) patients died during hospitalization • Risk factors for hospital mortality: • APACHE II OR=1.24 • Prior antibiotics OR=4.05 • Delay in Rx >12 hr OR-2.09 Morrell M, et al. Antimicrob Agents Chemother 2005;49:3640-45
BSI 8th 7th 6th 5th 4th 3rd 2nd 1st UTI 8th 7th 6th 5th 4th 3rd 2nd 1st Ranking of Fungal Infection NNIS System Report 1990 - 1999 Candida spp. S. aureus E. coli Other isolates
Management of Candiduria • Acquisition: GI or GU tract >hematogenous • Risk factors: indwelling urinary catheters, antimicrobial therapy • Differentiating infection from colonization is difficult: • Infection is commonly asymptomatic • Pyuria is very common in catheterized patients • Presence of pseudohype or colony counts do not help • Ascending infection: obstruction or instrumentation • Candidemia: usually brief and low grade; <5% risk
Sobel JD, et al. Clin Infect Dis 2000;30:19-24. • R, DB trial; compared fluconazole to placebo • 316 patients with candiduria and minimal or no symptoms • Rate of eradication FLU vs. placebo: • Overall: 50% vs. 29% • 14 days of Rx and no catheter: 78% vs. 47% • Candiduria 14 days after Rx: 32% vs. 35% Kaufman CA, et al. Clin Infect Dis 2000;30:14-8. • Prospective, MC, observational study • 861 patients with funguria, almost all asymptomatic • Resolution of funguria: • No antifungal Rx 76% • Catheter removal 35% • FLU or AMB bladder wash 50%
Management of Asymptomatic Candiduria • Asymptomatic candiduria rarely requires antifungal therapy: • Should not be treated unless neutropenia, low-birth weight, or urinary manipulation are present • Antifungal Rx is associated with rapid recurrence • No survival benefit • Same probability of clearing Candida as catheter removal • Focus on reducing the risk of Candida acquisition • Remove catheters and prosthetic stents • Limit antibacterial therapy • Treat whenever symptomatic, upper tract involvement, or hematogenous dissemination