Download
1 / 47
500 likes | 1.03k Views
Neuromuscular Emergencies. Hanni Bouma R3 Neurology. Outline. Approach to neuromuscular respiratory failure Signs & Symptoms Investigations Knowing when (to ask someone else) to intubate Overview of: Myasthenic crisis GBS Botulism. True or false? Regarding GBS…

E N D
Neuromuscular Emergencies Hanni Bouma R3 Neurology
Outline • Approach to neuromuscular respiratory failure • Signs & Symptoms • Investigations • Knowing when (to ask someone else) to intubate • Overview of: • Myasthenic crisis • GBS • Botulism
True or false? Regarding GBS… • ~10% of pts will require intubation. • All cases of suspected GBS should be treated with either IVIG or PLEX. • Normal CSF protein precludes the diagnosis. • Hypertension is the most common autonomic complication.
Case 1 • A 32-yo M with MG since age 20, on stable dose of pred 40, Imuran, and Mestinon, is admitted to hospital for elective bowel surgery (complications of diverticulitis) • Pt. has persistent diplopia and mild fatigable weakness at the deltoids • The surgery team calls you the morning of his scheduled surgery to ask if they should do anything for his myasthenia.
Case 1 • You should: • A) Suggest switching to equivalent dosage of IV steroids while NPO • B) Review med list & advise re: drugs that might trigger a crisis (ie. Antibiotics!!) • C) Kindly recommend postponing the surgery for pre-op IVIG or PLEX • D) All of the above
Case 2 • A 10-month-old infant presents with constipation and poor feeding followed by progressive hypotonia, descending weakness, dilated pupils, and bilateral ptosis. • What is the likely diagnosis? • How was it likely acquired? • How would you treat him?
Case 3 • You are called to see a patient in ICU with known diagnosis of MG, recurrent crises leading to ICU admissions, on stable dose of pred 60 mg qd and Imuran. Admitted with MG crisis, intubated then trach’ed. Now, 2 weeks later, “doing better” as per ICU. They want to start tapering his prednisone. What do you advise them to do?
Case 3 • 1) Agree with their plan to begin a slow tapering course by 10 mg qweek initially. • 2) Discuss the patient with their treating neurologist. • 3) Advise them to avoid rapid tapering of steroids given the risk of recurrent crisis. • 4) Both 2 & 3.
Respiratory Failure Basics • Type I:Hypoxia without hypercapnia • Usually associated with ↑ WOB • V/Q mismatch most common • Vascular disease/shunts (PE, Pulm. HTN, R->L shunts) • Interstitial lung disease (ARDS, cardiogenic pulmonary edema, pneumonia) • Pneumothorax, atelectasis
Type II: Hypercapnia with or w/o hypoxia • A.k.a. hypoventilation • Neuromuscular conditions • Deformities (kyphoscoliosis) • Reduced breathing effort (extreme obesity, drug effects, brainstem lesion affecting respiratory drive) • Increased airway resistance (asthma, COPD)
Neuromuscular Causes • Spinal cord lesion • Cervical cord compression, transverse myelitis • Motor neuron lesion • ALS • Peripheral nerve lesion • GBS, CIDP, critical illness polyneuropathy, Lyme disease, tick paralysis, toxic • NMJ disorder • MG, LEMS, botulism, organophosphate poisoning • Muscle lesion • Polymyositis, dermatomyositis, critical illness myopathy, hyperthyroidism, congenital myopathy (muscular dystrophy), mitochrondrial myopathy
History • Time course? • progressive weakness over hours to days GBS • fluctuating weakness (on an hourly basis) present for weeks/months MG • Distribution of weakness? • Proximal > distal (MG & GBS) • Ascending in GBS • Sensory Sx.? • Distal paresthesias common in GBS • No sensory inv’t in MG
History • +FH? • Pain? • Low backache frequently in GBS; neck pain: C-spine lesion? • Antecedent illness? • 60% of GBS triggered by viral URT illness or C.jejuni gastro • 40% of myasthenic crises triggered by infection • Medications • Exposure to fertilizers & pesticides? • Organophosphate poisoning • Recent diet • Botulism from home-canned goods
Exam • Long, thin face? (myotonic dystrophy? Congenital?) • Skin rash (dermatomyositis? • CNs • Pupils: • Reactivity may be lost in botulism or Miller-Fisher variant of GBS • EOM: • Opthalmoparesis or ptosis (MG? mitochondrial D/O? MFS?) • Presence or absence of bulbar weakness? • Motor exam: • Fasciculations? (ALS, organophosphate poisoning); tone; power (fatigable weakness? Distribution proximal vs. distal?)
Exam • Sensory: • Normal in MG • Distal sensory loss in GBS, esp vib/prop • Sensory level at C-spine level w/ quadriparesis = C-spine lesion • Coordination: • Ataxia in MF variant of GBS • Reflexes: • Areflexia in GBS; preserved in MG
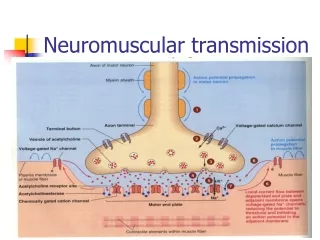
Mechanisms 1) Bulbar dysfunction: • Facial, oropharyngeal, laryngeal weakness upper airway obstruction in supine position • Impaired swallowing aspiration 2) Inspiratory muscle weakness/diaphragmatic paralysis atelectasis V/Q mismatch hypoxia 3) Expiratory muscle weakness hypoventilation AND weak cough/poor secretion clearance aspiration, pneumonia 4) Acute complications PE
Symptoms • If subacute (ie. GBS): dyspnoea and orthopnoea • Easy to overlook • If gradual onset, inadequate respiration usually occurs first during sleep • Symptoms of nocturnal hypoventilation: • a broken sleep pattern, nightmares, nocturnal confusion, morning headache, daytime fatigue, mental clouding and somnolence. • SOBOE less common in NMDs than in those with other Cardioresp D/O (reduced mobility) • Dyspnoea when lying flat or immersed in water • suggests weakness of the diaphragm
Warning signs • Rapid, shallow breathing • Stridor • Bulbar weakness • weak cough, nasal voice, pooling of saliva • Orthopnea • Staccato speech • Abdominal paradox • http://www.youtube.com/watch?v=RFGzdNFuXIM • Weakness of neck & trapezius muscles • Single-breath count Mehta, S. “Neuromuscular disease causing acute respiratory failure.” Respiratory Care, 2006. 51 (9): 1016-1023.
Investigations • Bedside PFTs:“20/30/40 rule” • Vital capacity (max exhaled volume after full inspiration). Normal = 60 ml/kg (4 L in 70 kg person). VC < 20 ml/kg (or 1 L) means intubation • Max inspiratory pressure. Index of ability to avoid atelectasis. Normal = > 80 cm H2O (male), >70 cm H2O (female). MIP >-30 means intubation • Max expiratory pressure. Index of ability to cough/clear secretions. Mean MEP = 140 cm H2O (male), 95 cm H20 (female). MEP <40 means intubation
Investigations • ABG: • Hypercarbia (PCO2 > 45 mmHg) • PCO2 often normal or low until late in NM resp failure • Established resp failure from NMDs: low pO2, normal pH, elevated bicarb & pCO2 • Elevations of bicarb & pH with normal pO2 & pCO2 suggest nocturnal hypoventilation • Hypoxia (PO2 < 75 mmHg) = usually atelectasis or pneumonia in acute setting • Basic labs (CBC, SMA-10, LFTs, CK) • CXR
Predictors of need for MV • 20/30/40 rule • or reduction in VC, MIP, MEP by >30% • PO2 <70 mmHg on RA or PCO2 >50 mmHg w/ acidosis • Dysarthria, dysphagia, impaired gag reflex
Intubation: things to think about • Code status? • Call ICU if signs of imminent resp failure • Identify early to avoid emergency intubation…elective intubation always preferred • Minimizes atelectasis/pneumonia • Minimizes complications of intubation specific to NMDs • Avoid depolarizing NM blockers
NPPV? • Few studies on its use in GBS & MG • Inappropriate if upper airway function severely impaired • More often used in chronic NMDs (ALS, muscular dystrophies) for chronic hypoventilation
General care • Serial PFTs (MIP/MEP/FVC) bid to qid • Electrolytes: low potassium, high magnesium & low phosphate exacerbate muscle weakness • Chest physio, suctioning & incentive spirometry • DVT prophylaxis • HOB elevation • NPO if bulbar weakness; NG or Dobhoff feeding
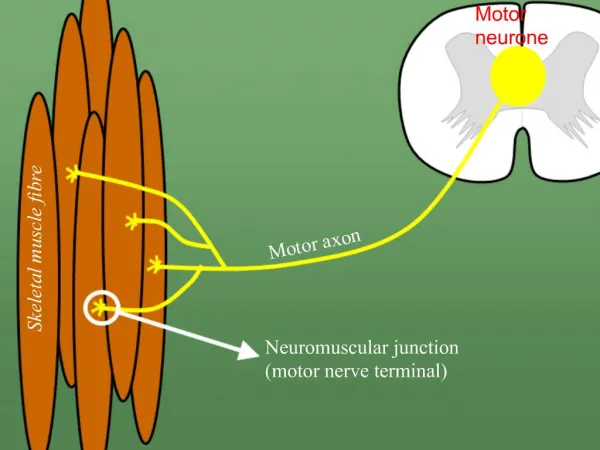
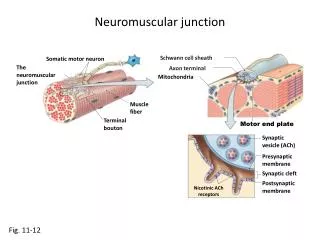
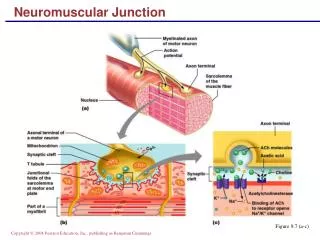
MG • Ab-mediated attack on nicotinic Ach rec defective transmission across NMJ • Bimodal: F 20-30 yo; M 50-60 yo • 2 autoimmune forms • Ach receptor Ab+: 80% with generalized MG & 50% with ocular MG • Anti-MuSK Ab+: 50% of patients who are Ach rec Ab negative; typically female with prominent bulbar weakness
Presentation • Motor: • Fluctuating, fatigable weakness involving eyes (90%), face/neck/oropharynx (80%), limbs (60%) • Limbs rarely affected in isolation • Rest restores strength (at least partially) • Sensory: normal • Reflexes: preserved • Thymic abnormalities: • Malignant thymoma in 10-15% (more severe disease) • Thymic hyperplasia in 50-70%
Investigations • Ach receptor Abs • Anti-MuSK Abs • Edrophonium (Tensilon) test: obsolete • EMG: • Repetitive nerve stimulation: >10% decrement in amplitude betw 1st & 5th CMAP • Single-fiber: “jitter” • Sens >95% for MG but not specific
Management: general • Symptomatic therapy (mild-moderate weakness): • Cholinesterase inhibitors (Mestinon) • Short-term disease suppression: • To hasten clinical improvement in hospitalized pts w/ crisis or impending crisis; pre-operatively; chronic refractory disease • PLEX or IVIG • Long-term immunosuppression: • When weakness is inadequately controlled by Mestinon • Prednisone • Azathioprine (if steroid failure or excessive SE) • Cyclosporine, Mycophenolate mofetil…
Myasthenic Crisis • Defined by resp failure requiring ventilatory assistance • Occurs in 20-30%; mortality 5% • Common precipitants: • Infection in 40% (esp respiratory) • Medications • Surgery • Pregnancy • Aspiration
Antibiotics: (**Penicillins like Tazocin are OK!) Aminoglycosides (genta, tobra) Fluroquinolones (cipro) Macrolides (erythromycin, azithro, tetracycline, doxycycline) Cardiac: All beta-blockers Calcium channel blockers Anticonvulsants: Phenytoin, CBZ Antipsychotics, lithium Thyroid hormones Magnesium toxicity Iodinated contrast agents Muscle relaxants Baclofen Long-acting benzos **Too much anticholinesterase Drugs that exacerbate MG
Myasthenic crisis: management • General • Determine if resp failure is imminent!! • Stop any meds that may be contributing • Mestinon usually stopped as well • May contribute to increased airway secretions in intubated patients • Treat any infection
Myasthenic Crisis: management • Specific • PLEX or IVIG: • start one or the other, quickly • Comparable efficacy • Evidence somewhat limited…TBD later • Earlier response seen with PLEX, but more adverse events • Preference somewhat individualized…
Myasthenic crisis: management • PLEX • Removal of anti AChR and antiMuSK Abs • 1 session/day x 5 • No superiority of PLEX qd x 5 vs qod x 5 • Rapid onset of action (3-10 days) • Need central line with associated complications • PTX, hemorrhage, line sepsis • Caution in pts with sepsis, hypotension; may lead to increased bleeding and cardiac arrhythmias
Myasthenic crisis: management • IVIG • 0.4g/kg/day x 5 days • Easily administered and widely available • Long duration of action • May last as long as 30 days • Side effects • Anaphylaxis in IgA deficiency • Renal failure, pulmonary edema • Aseptic meningitis • Thrombotic complications and stroke
Myasthenic crisis: management • Therapeutic effect of PLEX & IVIG is short-lived…lasts weeks • Therefore, glucocorticoids started at high dose (60 to 80 mg qd) as well • Onset of benefit at 2-3 wks, peaks at 5.5 mos • Initiation ass’d with transient worsening of weakness, serious in up to 50% • Occurs 5-10 days after initiation & lasts 5-6 days • Resp failure requiring MV in up to 10% • Concomitant use of PLEX or IVIG helps to prevent this transient worsening
GBS • Most common cause of acute or subacute gen’d paralysis • Monophasic AIDP: autoimmune attack against surface antigens on peripheral nerves • Develops 5 days to 3 weeks after resp/GI infection in 60% • Campylobacter jejuni (26%) • Viral URTI, influenza • EBV, CMV, VZV, HIV, hep A & B, coxsackie • Other precipitants: immunization, pregnancy, surgery, Hodgkin’s disease
Presentation • Sensory: • distal paresthesias/numbness (earliest Sx.) • Reduced vibration/proprioception • Motor: • Symmetric; evolves over days to 1-2 wks • Ascending: LE before UE; proximal> distal • Reflexes: reduced, then absent • Autonomic instability • Other: low backache very common, myalgias
Investigations • NCS/EMG: • Reduced conduction velocities • Loss of F waves • Conduction block in motor nerves • Reduced motor amplitudes: 2° axonal damage worse Px. • CSF: • High protein (may be normal in first 2 days) • No cells or few lymphs • 10% have 10-50 lymphs
Management • Admit for observation (potential for deterioration) • Determine if resp failure imminent • IVIG (0.4g/kg/d x 5 d) or PLEX (4-6 Rx. q1-2d) • Equally effective (2012 AAN guideline) • PLEX useful in first 2 weeks; benefit less clear after that…also more adverse effects • Steroids no proven benefit
Predictors of need for MV in GBS • Time from onset to admission < 7 days • Inability to cough • Inability to stand • Inability to lift elbows or head • LFT increases • Presence of autonomic dysfxn Sharshar T, Chevret S, Bourdain F, Raphael JC. Early predictors of mechanical ventilation in Guillain-Barre´ syndrome. Crit Care Med 2003;31(1):278–283.
Course • Progression over 1-4 weeks • Recovery: few wks to months • Mortality 3-5% • Poor prognosis: • Resp failure requiring intubation • Advanced age • Very low distal motor amplitudes (axonal damage) • Rapidly progressive weakness over 1 week
Botulism • Toxin is a presynaptic blocker of Ach release • Onset of Sx. 12-36 hours after ingestion • Prodrome: N/V, abdo pain, diarrhea, dry mouth • Symmetric neurologic deficits • First develop acute cranial neuropathies (opthalmoplegia, can be total; B/L ptosis, dysphagia, dysarthria, facial weakness) • Blurred vision secondary to pupillary dilatation • Descending muscle weakness • No sensory deficits apart from blurred vision • Urinary retention/constipation (smooth muscle paralysis) • Respiratory failure is primary cause of death
dry mouth diplopia dilated pupils droopy eyes droopy face diminished gag reflex dysphagia dysarthria dysphonia difficulty lifting head descending paralysis diaphragmatic paralysis “Dozen Ds” of Botulism
Botulism • Investigation: • Foodborne: serum analysis for toxin by bioassay in mice • Analysis of stool, vomitus, and suspected food items may also reveal toxin • Infantile: isolation of C.botulinum spores & toxin detection in stool • EMG • Treatment: • Equine serum heptavalent botulism antitoxin • Children older than 1 year of age and adults • Human derived botulism immune globulin (BIG-IV or BabyBIG) • Infants less than 1 year of age
Key points • 20/30/40 rule • Identify pts at risk for resp failure EARLY to avoid emergency intubation • Don’t wait for pts to complain of dyspnea before doing bedside PFTs