Download
1 / 21
230 likes | 419 Views
PHYSIOLOGIC CHANGES OF PREGNANCY. John G. Gianopoulos, M.D. Introduction.

E N D
PHYSIOLOGIC CHANGES OF PREGNANCY John G. Gianopoulos, M.D.
Introduction “During pregnancy, multiple physiologic adjustments are made to maintain maternal hemostasis. In a non-pregnant patient, many of these alterations would be considered pathologic rather than physiologic. This lecture will present the adjustments and alterations in maternal physiology.”
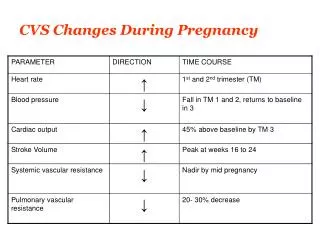
CardiovascularCardiac Output-is during pregnancy 1.51/min. Cardiac Output = heart rate x stroke volume. CO = HR x SV Output can be measured using direct Fick method, i.e.: Output of L. ventricle = 02 consumption (ml/min) A02 – V02
Pulse rate from 70 85 Heart rate by catecholamines Chromotropic Inotropic Stroke volume increases 10%. Regulated by 2 mechanisms. Heterometric Homometric CO, by SV = heart size
Mean arterial pressure - average pressure throughout cardiac cycle – decreased.Total peripheral resistance – dependent upon arteriole diameter – ie., small changes in caliber = large changes in TRP. R = 8hLr4During pregnancy TPR is reduced.
Increased blood flow – distribution. Uterus* Kidney Skin BreastsPulmonary Pressure – same as non-pregnant levels, due to: resistance to flow – vascular dilation volume – capacitance Radiographic appearance – increased vascularity, enlarged pulmonary vessels.
Venous Pressure - in femoral pressure: Weight of uterus of iliac veins, inf. Vena cava. Hydrodynamic obstruction – due to uterine outflow. Supine Hypotensive syndrome.
ECG Changes-elevation of diaphragm heart moved upwards and rotated forward, + enlarged. Therefore, one would predict change in the electrical axis of the heart. Deviation to the left in the electrical axis (15-28).
Volume and Composition of Blood.Plasma volume 40-50% RBC – 25-30% Hematocrit Fibrinogen Sedimentation rate Clotting Factors (VII, VIII, IX, X) Serum alkaline phosphatase
RESPIRATIONDefinitionsTital volume (TV) - amount of air moving into lungs with each inspiration. Inspiratory Reserve Volume (IRV) – air inspired with maximal inspiratory effort in excess of tidal volume. Expiratory Reserve Volume (ERV) - volume expelled by active expiratory effort after passive expiration. Residual Volume (RV) – air left in lungs after maximal expiratory effort.
Vital Capacity – greater amount of air that can be expired after maximal inspiratory effort. (timed vital capacity) Respiratory Minute Volume (RMV) – amount of air inspired/minute. Maximal Voluntary Ventilation – maximal amount of air that can be moved into and out of the lungs in one minute by voluntary effort.
During Pregnancy the following occurs: TV RMV – 40 %Hyperventilation Respiratory alkalosis – compensated Alveolar CO2 40mm Hg 30mm Hg sensitivity of brain stem respiratory centers to pCO2 – progesterone.
RENALPHYSIOLOGIC CHANGES: Renal Plasma Flow (RPF) - equals the amount of a substance excreted/unit of time divided by renal arteriovenous difference. (PAH,DIODRAST) RPF = U [x] V P [x] Renal blood flow – RPF x 1________ 1-hematocrit RPF is raised throughout pregnancy by 200-250 ml/1-min.
Glomerular Filtration Rate (GRF) - of plasma perfusing the glomeruli-about 20% reaches the tubular system of the kidney as an ultrafiltrate-i.e., GFR. GFR = U [x] V = Clearance P [X] ↑ creatinine clearance ↑ urea clearance ↑ uric acid clearance
Tubular Function: Na+Excretion-progesterone inhibits reabsorption, however, increasing aldosterone levels counteract this effect. H20=although plasma osmolality is ↓ and ECF ↑, urine volumes are similar to nonpregnant volumes. Hypothalamic resetting of osmoreceptors. Glycosuria-normal in pregnancy. Aminoaciduria-due to high circulating levels of cortisol?
↑ activity of renin-angiotensin- dissociation between pressor and renal effects. ↑ aldosterone ↑ erythropoietin
GASTROINTESTINAL Decreased motility, delayed absorption ↓ gastric secretion, ↓ tone of cardiac sphincter (reflex esophagitis)
ENDOCRINE STEROIDS: Progesterone-corpus luteum, fetal-placental unit. hyperpolarization of smooth muscle membrane potential- tone. ↑ temperature ↑ respiratory rate combined actions breast development
Estrogens-ovarian, fetal-lacental unit combined actions with progesterone connective tissue effects liver-binding globulins ↑, serum enzymes ↑.
PROTEIN HORMONES: HCG-human chorionic gonadotrophin-syncytial trophoblast corpus luteum diagnosis of pregnancy fetal adrenal hPL-human placental lactogen-syncytium GH like activity diabetogenic HCT-chorionic thyrotropin TSH like activity
PITUITARY HORMONES:Anterior Lobe ADH, Oxytocin ADRENAL HORMONES: Cortisol-increases Aldosterone-increases PANCREAS - ↑/s cell function, placental insulinase