Download

1 / 18
260 likes | 611 Views
Combination Antifungal Therapy. By Amy Barnett, Doctor of Pharmacy Candidate University of Florida College of Pharmacy. Fungal Infections: high risk populations. Neutropenic patients Solid organ transplant patients Diabetes Patients Immunocompromised Intensive care populations

E N D
CombinationAntifungalTherapy By Amy Barnett, Doctor of Pharmacy Candidate University of Florida College of Pharmacy
Fungal Infections: high risk populations • Neutropenic patients • Solid organ transplant patients • Diabetes Patients • Immunocompromised • Intensive care populations • Premature infants • Surgical populations
Most common fungal pathogens • Candida • Aspergillus • Cryptococcus
Antifungal Classification • Azoles • 1st gen: fluconazole, itraconazole, ketoconazole • 2nd gen: voriconazole • Polyenes • Conventional AmphoB (Amphocin) • Liposomal AmphoB (AmBisome) • Colloidal AmphoB (Amphotec) • Lipid complex AmphoB (Abelcet) • 5-Flucytosine • Echinocandins • Caspofungin, anidulafungin, micafungin
Azoles • Mechanism • Inhibits ergosterol biosynthesis by inhibition of 14-a-demethylase • Adverse effects • Nausea; diarrhea; abdominal pain; rash; edema; CHF; pulmonary edema; inc LFTs • Spectrum • Fluconazole: candida (not C.krusei), cryptococcus neoformins, histoplasma capsulatum • Itraconazole: above + aspergillus, coccidiodes immitis, paracocciodes, blastomycosis • Voriconazole: aspergillus, fusarium, scedosporium apiospermum, candida
Polyenes • Mechanism • Binds directly to ergosterol to alter cell membrane activity • Adverse effects • Fever, chills, phlebitis, anaphylaxis • give APAP and benadryl prior to infusion • Increased creatinine (prevention:saline load), hypokalemia (prevention:IV K+ replacement or amiloride 5-10mg/day), renal tubular acidosis • Spectrum • Broad spectrum: active against most fungal pathogens
5-flucytosine • Mechanism • FU FUTP inhibits protein synthesis • FU FUM interfere with DNA synthesis • Adverse effects • Bone marrow suppression, CNS effects, GI upset, rash, inc LFTs, inc SCr/BUN • Spectrum • Systemic candidiasis, cryptococcus • Used synergistically with AmphoB • Rapid resistance when used alone • Excellent CNS penetration
Echinocandins • Mechanism • Non-competitive inhibitor of glucan synthase (critical component of the cell wall) • Adverse effects • Pain at injection site, inc LFTs, flushing • Spectrum • Aspergillus, candida
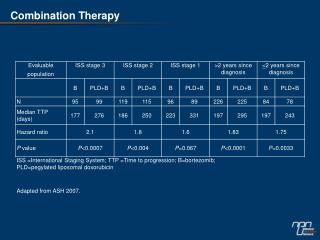
Studied Combinations • Fluconazole + Ampho B • Candidemia • Ampho B + 5-flucytosine • HIV-associated cryptococcal meningitis • Ampho B + fluconazole + 5-flucytosine • HIV-associated cryptococcal meningitits • Voriconazole + caspofungin • Aspergillus
Ampho B plus fluconazole • N=219 non-neutropenic pts with candidemia • Treatment groups: • Fluconazole + placebo • Fluconazole + AmphoB • Doses: fluconazole 800 mg qd +/- AmphoB 0.6-0.7mg/kg/day • Results: Combination therapy was not antagonistic and trended toward improved success (p=0.043) and increased eradication from the bloodstream (p=0.02). Rex, John H., Peter G Pappas, et al. Clin Inf Diseases 2003;36:1221-8
Selected antifungal drug interactions for Candida Table I. Combination In vitro In vivo Amphotericin B + flucytosine S, Add, I S, Add Amphotericin B + itraconazole Ant I, Ant Amphotericin B + fluconazole Add, I, Ant I, Ant Amphotericin B + terbinafine S, Add ND Amphotericin B + echinocandin S, Add, I I Amphotericin B + rifampicin S I Fluconazole + echinocandin I ND Flucytosine + fluconazole S, I, Ant S, Add, I Add = additive; Ant = antagonistic; I = indifferent; ND = insufficient data available; S = synergistic. Baddley, John W., et al. Drugs 2005;65(11):1461-1480
AmphoB + fluconazole + 5-flucytosine • N=64 pts • HIV-associated cryptococcal meningitis • Treatment Groups • AmphoB or • AmphoB + flucytosine or • AmphoB + fluconazole or • AmphoB + flucytosine + fluconazole • Dosing: AmphoB 0.7mg/kg/day; flucytosine 100mg/kg/day; fluconazole 400mg/day • Results: inc clearance with AmphoB + flucytosine regimen compared to AmphoB alone (p=0.006), AmphoB + fluconazole (p=0.02), or triple therapy (p=0.02). Brouwer, Annemarie E, et al. The Lancet 2004; 363:1764-1767.
Selected antifungal drug interactions for Cryptococcus Table II. Combination In vitro In vivo Amphotericin B + flucytosine S, I S, I Amphotericin B + itraconazole I S, I Amphotericin B + fluconazole S, I A, I Flucytosine + fluconazole S, Add, I S, I Add = additive; I = indifferent; S = synergistic. Baddley, John W., et al. Drugs 2005;65(11):1461-1480
Voriconazole + caspofungin • N=87 transplant pts with Aspergillosis • Treatment groups: • Voriconazole + caspofungin • AmphoB (as a control group) • Doses: voriconazole 6mg/kg q12h x 1 day, then 4mg/kg q12h; caspofungin 70mg/day x 1 day, then 50mg/day; AmphoB 5-7.4mg/kg/d. • Results: 90 day survival was significantly inc in transplant pts with renal failure (p=0.022) and those with A. fumigatus infection (p=0.019) compared to the control group. Singh, Nina, Ajit P Lamaye, et al. Transplantation 2006; 81(3): 320-326.
Selected antifungal drug interactions for Aspergillus Table III. Combination In vitro In vivo Amphotericin B + flucytosine S, Add, I S, Add, I Amphotericin B + itraconazole Ant Ant Amphotericin B + fluconazole I, Ant I Amphotericin B + terbinafine Add, I I Amphotericin B + echinocandin S, Add, I S, Add, I Amphotericin B + rifampicin S, I Add ExS triazole + echinocandin S, Add S, Add Amphotericin B + ExS triazole I ND Itraconazole + nikkomycin Z S ND Add = additive; Ant = antagonistic; ExS triazole = extendedspectrum azole (posaconazole, voriconazole or ravuconazole); I = indifferent; ND = insufficient data available; S = synergistic. Baddley, John W., et al. Drugs 2005;65(11):1461-1480
Advantages: Additive or synergistic effects Increased spectrum of activity Decreased resistance Disadvantages: Antagonistic effects Increased risk of drug interactions Increased toxicity Increased cost Advantages/Disadvantages of Combination Therapy Baddley, John W., et al. Drugs 2005;65(11):1461-1480
Conclusions • Severe infections • High risk patients • More studies with more combinations • More consistent results • Combinations with other AmphoB formulations • Micafungin + liposomal AmphoB (AmBisome) • Anidulafungin + lipid complex AmphoB (Abelcet)
References • Baddley, John W. and Peter G Pappas. Antifungal Combination Therapy: clinical potential. Drugs 2005; 65(11): 1461-1480. • Brouwer, Annemarie, Adul Rajanuwong, et al. Combination antifungal therapies for HIV-associated cryptococcal meningitis: a randomised trial. The Lancet 2004; 363: 1764-1767. • Kullberg BJ, JD Sobel, et al. Voriconazole versus a regimen of amphotericin Bfollowed by fluconazole for candidaemia in non-neutropenic patients: arandomised non-inferiority trial. The Lancet2005;366:1435-42. • Lacy, CF, et al. Lexi-Comp’s Drug Information Handbook. 13th ed. • Rex, John H., Peter G Pappas, et al. A randomized and blinded multicenter trial of high-dose fluconazole plus placebo versus fluconazole plus amphotericin B as therapy for candidemia and its consequences in nonneutropenic subjects. Clin Inf Diseases 2003;35:1221-8 • Singh, Nina, Ajit P Lamaye, et al. Combination voriconazole and caspofungin as primary therapy for invasive aspergillosis in solid organ transplant recipients: A prospective multicenter, observational study. Transplantation 2006; 81(3): 320- 326.