Download
1 / 39
390 likes | 533 Views
Pathophysiology of Combination Therapy in AMI. Combination Therapy. Reduces Reinfarction*. Thrombus. % Stenosis Minimum Diameter. Myocardial Blush ST Resolution. Epicardial Flow. Facilitates PCI. Myocardial Flow. *Gibson et al. J Am Coll Cardiol. 1995;25:582-589.

E N D
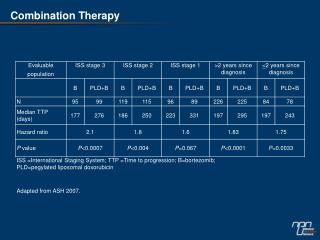
Pathophysiology of Combination Therapy in AMI Combination Therapy Reduces Reinfarction* Thrombus % Stenosis Minimum Diameter Myocardial Blush ST Resolution Epicardial Flow Facilitates PCI Myocardial Flow *Gibson et al. J Am Coll Cardiol. 1995;25:582-589. Gibson et al. Circulation. 2001;103:2550-2554.
Recent Clinical Trials GP IIb/IIIa Receptor Inhibitor Trial Lytic Anticoagulant GUSTO-V 100% r-PA 50% r-PA None Abciximab Standard-dose heparin Low-dose heparin ASSENT-3 100% TNK-tPA 50% TNK-tPA 100% TNK-tPA None Abciximab None ACC/AHA heparin dose Low-dose heparin Enoxaparin ENTIRE 50% TNK-tPA 50% TNK-tPA 100% TNK-tPA 100% TNK-tPA Abciximab Abciximab None None Unfractionated heparin Enoxaparin Unfractionated heparin Enoxaparin
Clinical Trials: Ongoing GP IIb/IIIa Receptor Inhibitor Trial Lytic Anticoagulant FASTER 50% TNK-tPA 75% TNK-tPA 100% TNK-tPA Tirofiban Tirofiban Tirofiban Low-dose heparin Low-dose heparin Low-dose heparin INTEGRITI 50% TNK-tPA 75% TNK-tPA 100% TNK-tPA Eptifibatide Eptifibatide Eptifibatide Low-dose heparin Low-dose heparin Low-dose heparin
GUSTO-I: A 20% Increase in TIMI Grade 3 Flow is Needed to Yield a 1% Mortality Reduction 60 54% 50 t-PA 6.3% 40 32% % TIMI Grade 3 Flow 30 20 SK 7.4% 10 0 t-PA SK 5 6 7 8 The GUSTO Angiographic Investigators. N Engl J Med. 1993;329:1615-1622.
TIMI Grade 3 Flow – Pooled Data From Dose Confirmation Phases of Recent Trials 100 Lytic alone Combination 78 80 73 73 70 64 60 56 56 54 54 % Patients With TIMI Grade 3 Flow 47 40 40 20 292 63 58 87 88 98 100 81 75 329 321 0 GUSTO-I 90 min T14 t-PA 90 min T14 r-PA 90 min SPEED 60-90 min INTRO-AMI 60 min Pooled 60-90 min
SPEED: Results of Dose-Confirmation Phase 100 TIMI-2 • There was a 7.4% improvement in the rate of TIMI Grade 3 flow • If a 20% improvement is required to improve mortality by 1%, then a 7.4% improvement would be predicted to improve mortality by 0.3% TIMI-3 80 28.7 21.6 60 Patency (%) 54.9 47.5 40 20 n=109 n=115 0 r-PA 10+10 U r-PA 5+5 U + Abx The SPEED Study Group. Circulation. 2000;101:2788-2794.
GUSTO-V: Study Design ST , lytic eligible, < 6 h (n=16,588) ASA No Abciximab Abciximab 2 x 10 U bolus (30’) Full-dose r-PA 2 x 5 U bolus (30’) Half-dose r-PA Standard Heparin: 5000 U bolus followed by800 U/h (< 80 kg) or 1000 U/h ( 80 kg) infusion Low-dose Heparin: 60 U/kg bolus followed by 7 U/kg/h infusion 1º end point: mortality at 30 days 2º end point: clinical and safety events at 30 days The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
Primary End Point: 30-Day Mortality 6 5.9% 5.6% 4 P=.43 for superiority % Mortality Non-Inferiority RR 0.95 (95% CI, 0.84-1.08) 2 Std. Reteplase (n = 8260) Abx + Dose Reteplase (n = 8328) 0 0 5 10 15 20 25 30 Days The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
GUSTO-V: Noninferiority Analysis Upper Boundary of 95% CI for Noninferiority 1.11 OR and 95% CI Non-Inferiority RR 0.95(95% CI, 0.84-1.08) 0.0 Abciximab + Half-dose r-PA superior 1.0 Full-dose r-PAsuperior 2.0 Adapted with permission from the GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
7.4% 5.9% A Comparison of the Outcomes With r-PA Monotherapy in GUSTO-III vs GUSTO-V Trials P<.001 P=.015 8 50 1.0 48% 0.91% 0.9 7 40 0.8 37% 6 0.7 0.59% 5 30 0.6 4 0.5 20 0.4 3 0.3 2 10 0.2 1 0.1 10,138 8,260 10,138 8,260 10,138 8,260 0 0 0 GUSTO III GUSTO V GUSTO III GUSTO V GUSTO III GUSTO V Death Anterior MI ICH The GUSTO-III Investigators. N Engl J Med. 1997;337:1118-1123. The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
GUSTO-V: Causes of Reinfarction 4 P<.0001 3.5 r-PA r-PA + Abx 3 2.7 2.3 Myocardial Infarction (%) 2 1.7 1.6 1.2 1 0.5 0.2 0 Any Q-wave Enzymatic Ischemic ST Change* *Unblinded, unadjudicated The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
Non-Intracranial Bleeding Through Discharge/Day 7 30 24.6 25 r-PA r-PA + Abx 20.0 20 % of Patients 15 13.7 11.4 10 5.7 5 4.0 3.5 1.8 1.1 0.5 0 Severe Bleeding Moderate Bleeding Mild Bleeding Any Bleeding Receiving Transfusions The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
ICH by Age Group 3 r-PA (n=8260) r-PA + Abx (n=8328) P=.069* 2.1 2 P=.53 1.5 % of Patients 1.2 1.1 1 P=.27* P=.66 0.5 0.4 0.4 0.3 37/7172 24/6230 21/6193 25/2030 31/2135 28/7179 12/1088 24/1149 0 70 yrs > 70 yrs 75 yrs > 75 yrs *Significant treatment interaction for the age 75 dichotomy; P=.033. The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
GUSTO-V: PCI Within 6 Hours (Urgent) and Through Day 7 * 30 27.9 * 25.4 25 20 Urgent PCI (%) 15 Through Day 7 * 10 8.6 * 5.6 5 0 r-PA r-PA + Abx *P<.0001. The GUSTO-V Investigators. Lancet. 2001;357:1905-1914.
GUSTO-V: Event Rates in Those Requiring Urgent PCI 12 r-PA n=1173 r-PA + Abx 10 9.6 9.0 8 6.7 Myocardial Infarction (%) 6 5.4 4.8 4 2.8 2 0 Death Repeat MI Death Plus Repeat MI Heartwire News. September 2, 2001. GUSTO-V: Combination half-dose fibrinolytic plus IIb/IIIa blocker. An Alternative approach to MI?
GUSTO-V: Conclusions • Compared with r-PA monotherapy, combination therapy with r-PA and abciximab resulted in • A mortality rate that was not inferior to r-PA monotherapy • Fewer nonfatal reinfarctions (primarily a reduced incidence of recurrent ST elevation) • A lower rate of urgent revascularization • More noncerebral bleeding complications, transfusions, and thrombocytopenia • A higher rate of ICH in elderly patients over the age of 75 years
ASSENT-3: Rationale for Use of Enoxaparin • TNK-tPA plus enoxaparin • Favorable effects of LMWHs in recent small-scale thrombolysis trials • Higher late patency: HART-2 ASSENT-Plus AMI-SK • Less reocclusion: HART-2 • Fewer reinfarctions: ASSENT-Plus AMI-SK Wilson, et al. • ASSENT-3 is the first large-scale trial to test LMWH
ASSENT-3: Study Design ST-Segment Elevation AMI (n=6095 patients) 150 to 325 mg ASA (daily) Randomized Full-dose TNK-tPAPlus Enoxaparin Half-dose TNK-tPAPlus AbciximabPlus Low-dose Heparin Full-dose TNK-tPAPlus Weight-adjusted UFH The ASSENT-3 Investigators. Lancet. 2001;358:605-613.
ASSENT-3: Primary End Points • Primary Efficacy End Point: Composite of 30-day mortality or in-hospital reinfarction or in-hospital refractory ischemia. • Primary Efficacy Plus Safety End Point: Composite of 30-day mortality or in-hospital reinfarction or in-hospital refractory ischemia plus in-hospital intracranial haemorrhage or in-hospital major bleeding other than intracranial.
ASSENT-3: 30-Day Mortality, Recurrent MI, Refractory Ischemia 3-way P=.0001 20 P=.0009* P=.0002* 15.4 15 11.4 11.1 10 % Risk of 30-Day D/MI/Ref Isch 5 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH *P-values are the Bonferroni P-values after correcting for multiple comparisons. The uncorrected P-values were P=.0002 for the enox vs UFH comparison, and P<.0001 for the abx vs UFH comparison.
17.0 ASSENT-3: 30-Day Mortality, Recurrent MI, Refractory Ischemia, Major Bleeding and ICH 3-way P=.0062 20 P=.0146* P=.057* 14.2 15 13.8 % Risk of 30-Day D/MI/Ref Isch/Maj Bleed/ICH 10 5 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH *P-values are the Bonferroni P-values after correcting for multiple comparisons. The uncorrected P-values were P=.0037 for the enox vs UFH comparison, and P=.0142 for the abx vs UFH comparison.
Kaplan-Meier Curves Primary Efficacy PlusSafety End Point Primary Efficacy End Point 20 20 18 18 UFH UFH 16 16 Abx 14 14 Enox* Enox* 12 12 Abx* 10 10 Probability (%) Probability (%) 8 8 6 6 4 4 log-rank P=.0001 *vs UFH log-rank P=.0062 *vs UFH + Abx 2 2 0 0 0 5 10 15 20 25 30 0 5 10 15 20 25 30 Days to death, reinfarction, orrefractory ischemia Days to death, reinfarction, refractoryischemia, ICH, or major bleeding Reprinted with permission from the ASSENT-3 Investigators. Lancet. 2001;358:605-613.
28.0 ASSENT-3: Primary Efficacy and Safety End Point of Death, Reinfarction or Refractory Ischemia, ICH or Major Bleeding in Patients >75 Years of Age 45 P=.001* 40 36.9 35 30 25.5 25 % Risk of 30-Day Efficacyand Safety End Point 20 15 10 5 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH *There was a statistically significant interaction between treatment with abciximab and age such that patients over the age of 75 had poorer outcomes with abciximab (P=.001).
16.5 ASSENT-3: Primary Efficacy and Safety End Point of Death, Reinfarction or Refractory Ischemia, ICH or Major Bleeding in Patients with Diabetes 30 P=.0007* 25 22.3 20 % Risk of 30-Day Efficacyand Safety End Point 13.9 15 10 5 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH *There was a statistically significant interaction between treatment with abciximab and diabetes, such that diabetics had poorer outcomes with abciximab therapy (P=.0007).
6.0 ASSENT-3: 30-Day Mortality 10 3-way P=.25 8 6.6 6 5.4 % Risk of 30-Day Mortality 4 2 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH
9.1 ASSENT-3: 30-Day Death or MI 10 3-way P=.0198 8 7.3 6.8 6 % Risk of 30-Day Death or MI 4 2 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH
4.2 ASSENT-3: In-Hospital Recurrent MI 5 3-way P=.0009 4 3 2.7 % Risk of In-HospitalRecurrent MI 2.2 2 1 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH
6.5 ASSENT-3: In-Hospital Refractory Ischemia 10 3-way P<.0001 8 6 % Risk of 30-DayRefractory Ischemia 4.6 4 3.2 2 0 TNK-tPA + Enox TNK-tPA + Abx TNK-tPA + UFH
ASSENT-3: Incidence of In-Hospital Thrombocytopenia and Noncerebral Bleeding Complications Enox Abx UFH P-Value (n=2040) (n=2017) (n=2038) 3-way Any thrombocytopenia 1.2 3.2 1.3 <.0001 Thrombocytopenia <.0001 <20,000 cells/µL 0.1 0.5 0.2 20,000 to 50,000 cells/µL 0.2 0.6 0.2 50,000 to 100,000 cells/µL 0.9 2.0 1.0 Bleeding episodes Total 25.6* 39.7 21.1 <.0001 Major 3.0* 4.3 2.2 .0005 Minor 22.6* 35.4 18.8 <.0001 Blood transfusion 3.4* 4.2 2.3 .0032 *While 3-way P-value is significant, Enox vs UFH comparison P=NS
Enox(n=2040) Abx(n=2017) UFH(n=2038) P-Value Total strokes 1.62 1.49 1.52 0.94 Intracranial hemorrhage 0.88 0.94 0.93 0.98 Ischemic stroke* 0.64 0.40 0.54 0.57 Hemorrhagic conversion 0.07 0.07 0.00 0.77 Unclassified 0.15 0.15 0.05 0.59 ASSENT-3: In-Hospital Stroke Rates *Including hemorrhagic conversion
Patients Undergoing PCI: Mortality ASSENT-3: In-Hospital PCI GUSTO-V: Urgent PCI 8 7 6.7 6 5.4 5 Mortality (%) 4 3.7 3 2.7 2.5 2 1 0 TNK-tPA +Enox TNK-tPA +Abx TNK-tPA +UFH r-PA +UFH r-PA +Abx
How Does Actual Weight Compare to Estimated Weight? Correlation Between Estimated and Actual Patient Weight in TIMI 10B 188.5 R2=0.93, P<.0001 Actual Patient Weight (kg) 40.5 36.4 181 Estimated Patient Weight (kg) Reprinted with permission from Cannon CP, et al. J Am Coll Cardiol. 2001;37:323A.
Weight-Based Dosing of Thrombolysis: How Well Do We Estimate Weight? How Often Would This Translate Into Errors With Administration of Thrombolytic Drugs and Adverse Outcomes? • Errors in estimating weight are uncommon, especially those that would lead to a dose change (1.3% or 49/3730 for TNK-tPA and 4.5% or 13/290 for t-PA). • No adverse outcomes were seen among patients who received an incorrect dose, suggesting a broad safety profile for the new single-bolus agent TNK-tPA. Cannon CP, et al. J Am Coll Cardiol. 2001;37:323A.
ASSENT-3: Study Group Conclusions Regarding TNK-tPA + Abciximab Therapy • “The results obtained with half-dose tenecteplase plus abciximab are very similar to those with half-dose reteplase and abciximab seen in GUSTO-V.” • “In both trials, these benefits are obtained at the cost of a higher rate of major bleeding complications and blood transfusions.” • “No benefit and perhaps even harm was observed in patients above 75 years and in diabetics.” • “Taken together they suggest that caution should be exercised regarding the use of conjunctive therapy with abciximab in elderly patients with an acute myocardial infarction treated with a fibrinolytic agent.” The ASSENT-3 Investigators. Lancet. 2001;358:605-613.
ASSENT-3: Study Group Conclusions Regarding Enoxaparin “In view of the present data and the ease of administration, enoxaparin might be considered an attractive alternative anticoagulant treatment when given in combination with tenecteplase.” The ASSENT-3 Investigators. Lancet. 2001;358:605-613.
ENTIRE TIMI-23: Study Design ST MI <6h (n=461) ASA Standard Reperfusion: Full-dose TNK-tPA(0.53 mg/kg) Combination Reperfusion: Half-dose TNK-tPA + Abx(0.27 mg/kg) UFH60 U/kg bolus12 U/kg/h infusion 36 h ENOXvarying doses+/- IV bolusIndex Hosp ( 8 d) UFH 40 U/kg bolus7 U/kg/h infusion 36 h ENOXvarying doses+/- IV bolusIndex Hosp ( 8 d) Antman E, et al. Eur Heart J. 2001;22:15. Abstract 145.
Outstanding Issues • Should enoxaparin replace UFH as the optimal antithrombin agent for AMI? • Will similar improvements in efficacy and safety occur if enoxaparin is combined with a less fibrin-specific agent such as r-PA? • Will physicians accept the use of enoxaparin in selected patients with ST-elevation MI who may require rescue PCI? • Will trials of TNK-tPA plus the small molecule GP IIb/IIIa receptor inhibitors produce results similar to ASSENT-3? • What is the optimal strategy for facilitated PCI?
Future Trials: Potential Downstream Targets • Large embolii: Filters • Small embolii (thrombii): Filters & GP IIb/IIIa inhibitors, p-selectin inhibitors • Vasoconstrictor release: GP IIb/IIIa inhibitors • Spasm: Adenosine, Ca channel blockers, alpha blockers, avoid over sizing with PCI, high pressure inflations, serotonin inhibitors, endothelin inhibitors • Endothelial & Myocardial swelling: Myocardial cooling, Ca channel blockers, DHEA, Na / H pump inhibitors, anti-inflammatory approaches