Download
1 / 37
450 likes | 970 Views
Brain stimulation lecture for medical students. Dr K Maaroganye Weskoppies Hospital 21 January 2013 . Brain stimulation therapies. 1) ECT 2) Deep brain stimulation 3) Transcranial magnetic stimulation 4) Vagal nerve stimulation. ECT Hollywood style: Dispel immediately . ECT.

E N D
Brain stimulation lecture for medical students Dr K Maaroganye Weskoppies Hospital 21 January 2013
Brain stimulation therapies 1) ECT 2) Deep brain stimulation 3) Transcranial magnetic stimulation 4) Vagal nerve stimulation
ECT • ECT remains the most effective Rx for MDD and a rapidly effective Rx for life-threatening psychiatric conditions. • A limiting variable in its use has been the adverse effect of confusion and memory loss associated with the course of treatment; however, both are reversible and new ECT technique seek to diminish cognitive effects while maintaining benefits.
Electrophysiology in ECT • A convulsion, or seizure, occurs when a large percentage of neurons fire in unison. • In ECT, seizures are triggered in normal neurons by application through the scalp of pulses of current, under conditions that are carefully controlled to create a seizure of a particular duration over the entire brain. • The ECT interictal EEG is generally slower and of greater amplitude than usual, but the EEG returns to preRx appearance 1 month to 1 year after the end of the course of treatment.
MOA • The induction of a bilateral generalized seizure is necessary for both the beneficial and the adverse effects of ECT but the exact MOA is unknown. • Theories • Degree of decrease in cerebral metabolism that takes place is correlated with therapeutic response • Virtually every neurotransmitter system is affected by ECT, but a series of ECT sessions results in downregulation of postsynaptic β-adrenergic receptors, the same receptor change observed with virtually all antidepressant treatments • Effects of ECT on serotonergic neurons remain controversial. Various research studies have reported an increase in postsynaptic serotonin receptors, no change in serotonin receptors, and a change in the presynaptic regulation of serotonin release • ECT has also been reported to effect changes in the muscarinic, cholinergic, and dopaminergic neuronal systems • In second-messenger systems, ECT has been reported to affect the coupling of G-proteins to receptors, the activity of adenylyl cyclase and phospholipase C, and the regulation of calcium entry into neurons ( mood-stabilizing drugs are being increasingly found to act on G proteins or other second messengers)
Indications: 1) MDD: ECT is the fastest and most effective available therapy. 70 % advantage ( failed drug trials) So which patients: Failed medication trials or have not tolerated medications Severe or psychotic symptoms Acutely suicidal or homicidal Marked symptoms of agitation or stupor. Who refuse to eat. Elderly patients who cannot tolerate antidepressants Suicidal pregnant patients who cannot take medication Previous good response to ECT Patient’s preference • ECT is a Rx for MDE and does not provide prophylaxis unless it is administered on a long-term maintenance basis.
Indications: 2) Manic Episodes: ECT is at least equal to lithium in the Rx of acute manic episodes. Drug rx for manic episodes, however, very effective in the short term and for prophylaxis So which patients: pts with C/I to all available mood stabilizers and those approaching dangerous levels of exhaustion 3) Schizophrenia: So which patients: Marked positive symptoms Catatonia( early ECT may prevent life-threatening C/S) Accompanying affective symptoms, are considered most likely to respond to ECT ( faster improvement)
Other indications • ECT is also reportedly useful to treat: Episodic psychoses, atypical psychoses, OCD, and delirium and such medical conditions as NMS , hypopituitarism, intractable seizure disorders, and the on-off phenomenon of Parkinson's disease.
Clinical Guidelines: • Clinicians must explain both beneficial and adverse effects and alternative treatment approaches. The informed-consent process should be documented in the patients' medical records and should include a discussion of the disorder, its natural course, and the option of receiving no treatment. • The use of involuntary ECT is rare today and should be reserved for patients who urgently need treatment and who have a legally appointed guardian who has agreed to its use. • Pretreatment evaluation should include standard physical, neurological, and pre-anaesthesia examinations and a complete medical history.
Consent • As far as possible, patients and their families should be involved in discussions. • Informed consent should be: in writing detail the procedure express indications for treatment explain risks and adverse effects( esp older pts, pregnant and young pts) offer alternative forms of treatment explain risks of no treatment
Existing GMC • Any physical illness will need to be investigated and treated or at least stabilised as far as possible before ECT is begun. An anesthetist opinion should be sought. • Higher cardiac risks during treatment esp in pts : recent MI, severe valvular heart disease, clinically significant cardiac dysrhythmias, unstable angina, uncompensated CFF and some aneurysms • CNS conditions: ECT has been used safely for people with small, slow-growing cerebral tumours without raised ICP , but people who have SOL of the brain are at high risk of neurological deterioration if treated with ECT. Nevertheless, other neurological conditions( including those with strokes and learning disabilities) have been treated successfully with ECT. • Other medical conditions to be considered : oesophageal reflux (increased risk of aspiration), diabetes( Rx may need to be modified), people with bone or joint disease( may need an increased dose of muscle relaxant, although fracture during ECT has been virtually eliminated with the use of muscle-relaxant drugs, advanced glaucoma( seek ophthalmological advice) • Always minimize risk in the above pts( in-pt ECT, liaise with anesthetist , get staff who are proficient in resuscitation, ECT close to high care unit) • On the occasions when ECT is prescribed to save life, there may be no absolute contraindications to it.
Physical exam • To expose any evidence of cardiac failure, severe valvular disease or unstable dysrhythmia, uncontrolled HT, significant infection, poor dentition, obesity, marked cachexia or factors that might prejudice airway mx, such as arthritis, particularly of the neck or jaw. • BP, weight and urinalysis should be recorded.
Pre ECT inx Any of the following may be performed, but only as clinically indicated: • FBC– on most patients • U&E – for patients taking lithium, diuretics or other vasoactive/cardiac drugs, those with diabetes and those with renal disease • LFT – on patients with cachexia, a history of alcoholism, drug abuse or recent overdose • INR– for patients taking anticoagulants • hepatitis B antigen status – on known drug abusers • Blood glucose levels – if urinalysis is positive • ECG – on patients with known cardiovascular, respiratory or renal disease, irregular pulse or heart murmur, hypertension, those with diabetes aged over 40, and all patients over 50 • CXR – for patients with suspected chest infection, cardiomegaly, congestive cardiac failure, pulmonary embolism (PE) or who have had recent falls (because of the possibility of fractured ribs) • A pregnancy test – if appropriate.
Concomitant meds • The use of tricyclic and tetracyclic drugs, monoamine oxidase inhibitors, and antipsychotics is generally considered acceptable • Benzodiazepines used for anxiety should be withdrawn because of their anticonvulsant activity • lithium should be withdrawn because it can result in increased postictal delirium and can prolong seizure activity • Clozapine and bupropion should be withdrawn because they are associated with the development of late-appearing seizures • Lidocaine should not be administered during ECT because it markedly increases the seizure threshold • Theophylline is c/i because it increases the duration of seizures • Reserpine is also c/i because it is associated with further compromise of the respiratory and cardiovascular systems during ECT. • Decisions to be taken by prescribing psychiatrist.
Day of ECT • Nil per os • Unless specifically stated, all regular medications, with the exception of insulin, should be taken, not less than 2 hours before treatment, with sips of water if necessary • Otherwise no food for 6 hours and drink only moderate volumes of clear fluids until 2 hours before treatment • Diabetics - blood glucose estimate should be performed immediately before each treatment
Anaesthetics • The objective of anaesthesia: provide unconsciousness necessary to cover muscle relaxation, the electrical stimulus and resultant seizure. • Induction agents used at WKH is Propofol (0.75–2.5 mg/kg). It is thought to reduce seizure duration but improve cardiovascular stability. • Muscle relaxants used at WKH is Suxamethonium. They are meant to ameliorate the convulsive muscle activity during stimulation and the subsequent seizure and reduce the risk of injury. • The electrical stimulus should be applied only after fasciculations have ceased. • Bite block: The initial direct tetanic stimulation of the masseter by the electrodes leading to unavoidable maximal stimulation that presents the greatest danger to the patient’s dentition. • Record keeping and organisation: The doses of all anaesthetic agents used, the patient’s response, and monitor recordings before and immediately after treatment. This is pertinent info for future treatments. • Hyperventilation (approximately 20 breaths) immediately before the application of the electrical stimulus has been shown to enhance seizure duration.
Muscarinic Anticholinergic Drugs: • Muscarinic anticholinergic drugs are administered before ECT to minimize oral and respiratory secretions and to block bradycardias and asystoles, unless the resting heart rate is above 90 beats a minute • Atropine: 0.3 to 0.6 mg IM/SC 30 to 60 minutes before the anaesthetic or 0.4 to 1.0 mg IV 2 or 3 minutes before the anaesthetic • Alternative: glycopyrrolate
ECT seizure • A well-modified seizure will be manifest as minor tonic followed by clonic activity of skeletal muscle, accompanied by a typical seizure pattern on EEG. • ADEQUATE SEIZURE Generalized and tonic-clonic of 20-25 seconds duration peripherally and 30 seconds EEG recorded with Spike waves during tonic phase Spike and slow waves during the clonic phase and Seizure termination followed with post-ictal suppression • Cuff technique / EMG to objectively judge seizure duration
Number and Spacing of Rx: • ECT Rx are usually administered 2-3 times a week; twice-weekly Rx are associated with less memory impairment than thrice-weekly Rx. • In general, the course of Rx of MDD can take 6 to 12 treatments (although up to 20 sessions are possible) • Manic episodes can take 8 to 20 treatments • SZP can require more than 15 treatments • Catatonia and delirium can take as few as 1 to 4 treatments. • Rx should continue until the patient achieves what is considered the maximal therapeutic response. Further treatment does not yield any therapeutic benefit, but increases the severity and duration of the adverse effects.
Adverse Effects Cognitive impairments: There is great individual variability. Confusion: It can range from postictal and postanesthetic confusion of 30 minutes to severe agitation ( 5%). Symptoms include(disorientation, associated with impaired attention, memory and praxis).These effects resolve over time and are normally short-lived. Postictal delirium(rare): which can manifest as restlessness, aggression or agitation in the early stages of recovery. This will respond to treatment with benzodiazepines. Memory problems: ECT produces deficits in both autobiographical and impersonal memory domains/ retrograde and anterograde components. It diminishes as ECT administration becomes more remote. Bilateral treatments ( and more frequent ECT) are associated with significantly greater verbal memory impairment than nondominant hemisphere unilateral treatments. These losses improve substantially after completion of an ECT course. There are no pharmacological treatments.
Mortality rate • ECT is a low-risk procedure with a mortality rate similar to that of anaesthesia for minor surgical procedures, despite its frequent use in elderly people and those with major medical problems (Sackeim, 1998; Weiner et al, 2000). • Anaesthesia >death • Incidence in first 24h >1:24 000 • Most CVS complications / aspiration / brain herniation- patients identified as being at high risk should be closely monitored and treated in an environment that will allow rapid intervention should c/s occur • ECT is very safe none the less
Other adverse affects • Spontaneous Seizures: Incidence 0.1 - 0.5 % , related to underlying seizure disorders. Non-convulsive status epileptcus( presents with persistent confusion after ECT) • Fractures • Broken teeth • Back pain • “Scoline flu” • Nausea, vomiting • Headaches: - NSAID’s useful - migrainous headache > sumatriptan 25 mg orally - ergot compounds > exacerbate cardiovascular changes • Note: Regular review is necessary during the course of treatment to detect the possible adverse effects listed above. If detected, this should prompt consideration of whether these could be avoided, minimised or treated.
Brain damage? • Concern > structural damage to the CNS suggested by cognitive impairment • Presently no convincing evidence indicates that either ECT or intermittent brief seizures, such as those induced during ECT, produce structural damage to the brain • Based on careful and thorough reviews of the literature, including both human and animal studies, researchers conclude strongly that there is no evidence that ECT produces structural damage to the brain.
Contraindications • ECT has no absolute c/i, only situations in which a patient is at increased risk and has an increased need for close monitoring. • Pregnancy is not a c/i for ECT, and fetal monitoring is generally considered unnecessary unless the pregnancy is high risk or complicated. • Patients with SOL are at increased risk for oedema and brain herniation after ECT. If the lesion is small, however, pretreatment with dexamethasone is given, and HT is controlled during the seizure, and the risk of serious complications can be minimized for these patients. Patients who have increased intracerebral pressure or are at risk for cerebral bleeding (e.g, those with cerebrovascular diseases and aneurysms) are at risk during ECT because of the increased cerebral blood flow during the seizure. This risk can be lessened, although not eliminated, by control of the patient's blood pressure during the treatment. • Pts with recent Mi (4-6 weeks)are another high-risk group, although the risk is ↓2 weeks after the MI and is even ↓↓3 months after the infarction. Patients with HT should be stabilized on their antihypertensive medications before ECT is administered.
Post ECT treatment • Patients who have failed particular meds should not be treated again with those medications after they respond to ECT. Other AD’s with good response / never used before should be tried. • Continue treatment for 6 months at least at full dose. • Most contemporary patients treated with ECT suffer from recurrent illness and are likely to be candidates both for more intensive continuation treatment and for longer-term prophylactic treatment, to reduce the risk of future episodes of illness.
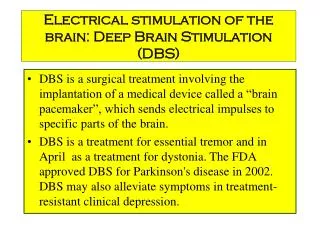
Deep brain stimulation • Deep brain stimulation (DBS) involves creating a small hole in the skull and passing a fine wire into selected brain regions. This wire can be excited on its terminal end by a pacemaker-like device connected subdermally and implanted in the chest wall. When the DBS is implanted, the wire stimulates at high frequencies and temporarily stops the function at that region • Used in PD,OCD and Tourette’s disorder.
Transcranial magnetic stimulation • Repeated transcranial magnetic stimulation (rTMS) is a noninvasive technique for stimulating cells of the cerebral cortex. It creates a time-varying magnetic field in which a localized pulse magnetic field over the surface of the head depolarizes the superficial neurons. • TMS uses a hand-held magnet to allow focused electrical stimulation across the scalp and cranium without the pain associated with percutaneous electrical stimulation). • MDD: PET scans have revealed a relative hypofrontality in some patients with MDD. It has been proposed that rTMS stimulation of these frontal areas would relieve symptoms of depression. The therapeutic effects of TMS take several weeks to consolidate, and thus may require several weeks worth of Rx. • rTMS has shown some preliminary efficacy in OCD and PTSD. • The procedure is considered to be safe and no cognitive, neurological or cardiovascular adverse events have been reported with its use. TMS appears safe, but the major serious concern is its causing a seizure.
Vagal nerve stimulation • VNS refers to stimulation of the left vagus nerve using commercially available devices. • The VNS is delivered through a bipolar pulse generator, which is multiprogrammable and implanted in the left chest wall through a bipolar lead. • It has been shown through brain imaging studies that VNS affects the metabolism of limbic structures that are involved in mood stabilization, and has neurochemical effects on brain monoamines, involved in regulation of depressed mood. • VNS was recently approved by the FDA as an adjunctive long-term treatment for patients with recurrent or chronic major depressive disorders who have failed at least four antidepressant medication trials. VNS did not seem to have any efficacy in severe treatment resistance. The VNS procedure does not seem to give adverse effects, with the exception of mild transient hoarseness in approximately 55 percent of patients.