Download
1 / 1
10 likes | 275 Views
“ Comparative evaluation of Laparoscopic Gastric Bypass (LGB) vs Adjustable Gastric Band (AGB) over 5 year period: Bypass or Band? ” Khan J MD, David C MD, Bani MGM MD, Haddad A MD, Singh K., MD FACS, Vonrueden D., MD FACS, Averbach A., MD FACS.

E N D
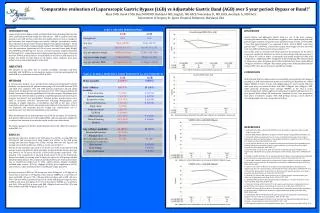
“Comparative evaluation of Laparoscopic Gastric Bypass (LGB) vs Adjustable Gastric Band (AGB) over 5 year period: Bypass or Band?” Khan J MD, David C MD, Bani MGM MD, Haddad A MD, Singh K., MD FACS, Vonrueden D., MD FACS, Averbach A., MD FACS. Department of Surgery, St. Agnes Hospital, Baltimore, Maryland, USA . DISCUSSION Gastric bypass and Adjustable Gastric band are one of the most common bariatric procedures today. The literature suggests a more rapid weight loss with gastric bypass. Patients are noted to lose anywhere between 50% to 77% EBWL 1 year after gastric bypass9,10 as compared to 30% - 52% of EBWL 1 year after gastric band.11-14 However, 3 years after surgery, total weight loss does not seem to be very different between the two procedures.15,16 Our results seem to correlate with those stated in the literature for the first 2 years post operatively. However, we notice an interesting trend between years 2 to 5 where we seem to notice a continuous and steady weight loss with AGB compared to a slight drop-off in weight loss in the LGB group. This trend seemed to remain even when the group was further subdivided into those with a BMI of <50kg/m2 and those >50kg/m2. Our patient groups were fairly equally divided in terms of M:F ratio, age, as well as pre-op BMI and weight. CONCLUSION Both LGB and AGB procedures show low morbidity and mortality with delayed morbidity in AGB increasing with duration of follow-up. LGB patients do exhibit higher %EBWL in first 1-2 years with weight regain at 5 years overall. This was seen even when we looked at those with BMI <50kg/m2 and >50kg/m2. AGB, while generally producing lower average %EBWL in the first 2 years, demonstrated more stable weight loss maintenance in patients followed over a 5 year period. While today LGB remains the “standard of care”, both procedures have place in bariatric surgery with AGB perhaps having a more stable & increasing weight loss over a longer period of time. REFERENCES 1. Santry HP, Gillen DL, Lauderdale DS (2005) Trends in bariatric surgical procedures. JAMA 294(15):1909–1917 2. Bennett JMH, Mehta S, Rhodes M. Surgery for morbid obesity. Postgrad Med J. 2007;83:8–15. 3. Cottam DR, Atkinson J, Anderson A, et al. A case-controlled matched-pair cohort study of laparoscopic Roux-en-Y gastric bypass and Lap-Band patients in a single US center with three-year follow-up. Obes Surg. 2006;16:534– 540. 4. Jan JC, Hong D, Bardaro SJ, et al. Comparative study between laparoscopic adjustable gastric banding and laparoscopic gastric bypass: single-institution, 5-year experience in bariatric surgery. Surg Obes Relat Dis. 2007;3:42–51. 5. Kim TH, Daud A, Ude AO, et al. Early US outcomes of laparoscopic gastric bypass versus laparoscopic adjustable silicone gastric banding for morbid obesity. Surg Endosc. 2006;20:202–209. 6. Biertho L, Steffen R, Ricklin T, et al. Laparoscopic gastric bypass versus laparoscopic adjustable gastric banding: a comparative study of 1,200 cases. J Am Coll Surg. 2003;197:536–547. 7. Bowne WB, Julliard K, Castro AE, et al. Laparoscopic gastric bypass is superior to adjustable gastric band in super morbidly obese patients: a prospective, comparative analysis. Arch Surg. 2006;141:683–689. 8. Galvani C, Gorodner M, Moser F, et al. Laparoscopic adjustable gastric banding versus laparoscopic Roux-en-Y gastric bypass: ends justify the means? Surg Endosc. 2006;20:934–941. 9. Schauer PR, Ikramuddin S, Gourash W, et al. Outcomes after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Ann Surg. 2000; 232:515–529. 10. Higa KD, Ho T, Boone KB. Laparoscopic Roux-en-Y gastric bypass: technique and 3-year follow-up. J Laparoendosc Adv Surg Tech A. 2001;11:377–382. 11. Rubenstein RB. Laparoscopic adjustable gastric banding at a U.S. center with up to 3-year follow-up. Obes Surg. 2002;12:380–384. 12. Belachew M, Legrand M, Vincenti VV, et al. Laparoscopic placement of adjustable silicone gastric band in the treatment of morbid obesity: how to do it. Obes Surg. 1995;5:66–70. 13. O’Brien PE, Dixon JB, Brown W, et al. The laparoscopic adjustable gastric band (Lap-Band): a prospective study of medium-term effects on weight, health and quality of life. Obes Surg. 2002;12:652–660. 14. Fielding GA, Rhodes M, Nathanson LK. Laparoscopic gastric banding for morbid obesity. Surgical outcome in 335 cases. Surg Endosc. 1999;13:550 –554. 15. Weiner R, Blanco-Engert R, Weiner S, et al. Outcome after laparoscopic adjustable gastric banding—8 years experience. Obes Surg. 2003;13: 427– 434. 16. Vertruyen M. Experience with Lap-band System up to 7 years. Obes Surg. 2002;12:569 –572. Table 1. PATIENT DEMOGRAPHICS . FIG 1. TRENDS IN OVERALL BMI COMPARING LGB AND AGB Table 2. OVERALL MORTALITY, EARLY MORBIDITY & LATE MORBIDITIY FIG 2. TRENDS IN OVERALL PERCENT ESTIMATED BODY WEIGHT LOSS COMPARING LGB AND AGB INTRODUCTION Laparoscopic Gastric Bypass (LGB) and Adjustable Gastric Banding (AGB) are the most commonly performed weight loss procedures1. AGB is a purely restrictive procedure and LGB involves restriction and malabsorption as well as changes to gut hormones that impact hunger and satiety2. Multiple retrospective studies have reported on the outcomes of gastric bypass versus gastric banding3-8. Initial enthusiasm with LAGB is being gradually replaced by significant disillusionment with this procedure. Opponents of LGB cite poor percent Excess Body Weight Loss (%EBWL) at follow-up over 2 years. A review and meta-analysis conducted by Buchwald et al . comparing open and laparoscopic bariatric surgery outcomes between 1990 to 2003 showed an overall %EWL of 47.5% for LAGB based on 12 studies and 61.6% for LGB based on 22 studies. These estimates have been widely used as clinical benchmarks in the field. OBJECTIVE The purpose of our study was to evaluate morbidity, mortality, long-term morbidity and %EBWL in a retrospective analysis of patients undergoing LGB and LAGB at our institution between 2005 to 2010. METHODS A retrospective analysis of our prospectively-maintained institutional bariatric database was performed. All patients undergoing LGB and LAGB between 2005 and 2010 were analyzed. 1471 and 1368 patients underwent LGB and LAGB, respectively. All patients met the requirements of the 1991 National Institute Of Health Consensus Conference guidelines3 for bariatric surgery. All patients were preoperatively screened and counseled by a multidisciplinary team involving the surgeon, nutritionist and psychologist. Detailed patient questionnaires were used to document patient's characteristics including demographics, past attempts at weight reduction, co-morbidities and BMI at the time of first consultation. Post-operatively, all patients were followed at the bariatric clinic at our institution and perpetual data for weight loss, complications and re-operations were recorded and maintained in our database. After identification of our patient groups overall 30 day mortality, 5yr morbidity, preoperative BMI and excess body weight (EBW), and post-operative weight loss at various time intervals as seen in the results section were determined. Our patient groups were further subdivided into those with a BMI >50 and those with a BMI <50. RESULTS Average pre-operative weight in the LGB group was 307lbs, average BMI was 49.8 kg/m2 and average excess body weight was 151lbs. In the AGB group average pre-operative weight was 275lbs, average BMI was 44.5 kg/m2 and average excess body weight was 120lbs as can be seen in table 1. Overall 30 day mortality was noted to be 0.07% and 0.0% in the LGB and AGB groups respectively (table 2). Early morbidity (occurring within 30 days post op) was noted to be 7% and 1.5% in the LGB and AGB groups respectively. This included 1.3% reoperations in the LGB group versus 0.3% in the AGB group. Delayed morbidity (occurring after 30 days post op) in the LGB group included intestinal obstruction (1.3%), marginal ulceration (2%) and revision procedures due to insufficient weight loss in (1%). LAGB patients delayed morbidity included band erosion (0.14%), slippage (0.65%), port complications (0.5%) and revision to other procedures due to insufficient weight loss (2%). Average decrease in BMI in LGB group was from 49.8kg/m2 to 32.6kg/m2 at 2years but an increase to 37.4kg/m2 at 5yrs (Fig 1). %EBWL at 1, 2 and 5yrs of those with BMI <50 were 74%, 74% and 62% and those with a BMI >50 were 59%, 62% and 46%, respectively (fig 3 & 4). In the AGB group average decrease in BMI in was from 44.5 kg/m2 to 37.7% in 5yrs (fig 1). %EBWL at 1,2 and 5yrs was 36%, 35% and 50% in those with BMI <50kg/m2 and was 28%, 35% and 40% in those with BMI >50kg/m2 (fig 3 & 4). FIG 3. TRENDS IN %EBWL COMPARING LGB AND AGB IN PATIENTS WITH BMI <50kg/m2 FIG 4. TRENDS IN %EBWL COMPARING LGB AND AGB IN PATIENTS WITH BMI >50kg/m2






