Download
1 / 9
90 likes | 101 Views
Learn about squamous and adenocarcinoma of the oesophagus, clinical features, diagnostic tests, staging, and treatment options.

E N D
Squamous oesophageal cancer is relatively rare in Caucasians (4/100 000), whilst in Iran, parts of Africa and China it is much more common (200 per 100 000). Squamous cancer can arise in any part of the oesophagus, and almost all tumours in the upper oesophagus are squamous cancers.
Adenocarcinomas typically arise in the lower third of the oesophaguswhy??The incidence is increasing and is now approximately 5:100 000 in the UK; this is possibly because of the high prevalence of gastro-oesophageal reflux and Barrett's oesophagus in Western populations.
Squamous carcinoma: aetiological factors1-Smoking 2-Alcohol excess 3-Chewing betel nuts or tobacco 4-Coeliac disease 5-Achalasia of the oesophagus6-Post-cricoid web 7-Post-caustic stricture 8-Tylosis (familial hyperkeratosis of palms and soles)
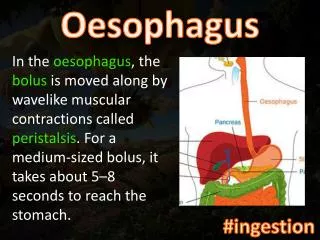
Clinical featuresMost patients have a history of progressive, painless dysphagia for solid foods. Others present acutely because of food bolus obstruction. In late stages weight loss is often extreme; chest pain or hoarseness suggests mediastinal invasion. Fistulation between the oesophagus and the trachea or bronchial tree leads to coughing after swallowing, pneumonia and pleural effusion.
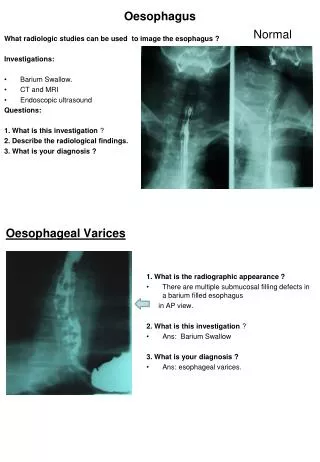
Investigations1. For diagnosis:-The investigation of choice is upper gastrointestinal endoscopy with cytology and biopsy.-A barium swallow demonstrates the site and length of the stricture but adds little useful information. 2. For staging: -Thoracic and abdominal CT are carried out to identify metastatic spread and local invasion.-Endoscopicalultrasound (EUS)is the most sensitive method for determining depth of penetration of the tumour into the oesophageal wall and for detecting involved locoregional lymph nodes. These investigations will define the TNM stage of the disease.
Adenocarcinoma of the lower oesophagus. in association with Barrett’s oesophagus (arrow).
TreatmentThe treatment of choice is surgery if the patient presents at a point at which resection is possible. Although squamous carcinomas are radiosensitive, radiotherapy alone is associated with a 5-year survival of only 5%, but combined chemoradiotherapy for these tumours can achieve 5-year survival rates of 25-30%.
Approximately 70% of patients have extensive disease at presentation; in these, treatment is palliative and based upon relief of dysphagia and pain.Endoscopic laser therapy or self-expanding metallic stents are used to improve swallowing. Quality of life can be improved by nutritional support and appropriate analgesia.