Download
1 / 57
570 likes | 1.09k Views
Study to Prevent Joint Disease In Young Children with Hemophilia New Hemophilia Therapies for Today and Tomorrow Marilyn J. Manco-Johnson, MD University of Colorado at Denver and Health Sciences Center March 9, 2006. Hemophilia: X-linked recessive

E N D
Study to Prevent Joint Disease In Young Children with HemophiliaNew Hemophilia Therapies for Today and TomorrowMarilyn J. Manco-Johnson, MDUniversity of Colorado at Denver and Health Sciences CenterMarch 9, 2006
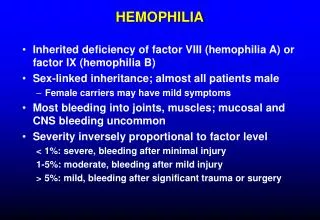
Hemophilia: X-linked recessive Affects 1:5000 live male births Causes deficient clotting FVIII activity Life-threatening hemorrhages Arthropathy causes most significant chronic morbiditiy
Subgaleal hematoma in a newborn infant with severe hemophilia
Extrinsic pathway Intrinsic pathway TF, VII TF, VIIa Initiation IX IXa IX VIIIa TF, VIIa X Xa Va Prothrombin Thrombin Fibrinogen Fibrin
Extrinsic pathway TF, VII Intrinsic pathway TF, VIIa XI XIa Amplification IX IXa IX VIIIa F VIII TF, VIIa X Xa Va F V Prothrombin Thrombin Fibrinogen Fibrin
Prophylaxis:Routine infusions of replacement clotting factor to prevent bleeding events Initial Observation:Persons with moderate hemophilia (1-5% FVIII) have decreased joint disease (Dr. Inge Marie Nilsson) Hypothesis:Converting a person from severe hemophilia to moderate with prophylaxis would decrease incidence of joint disease. Goal:To raise FVIII above 1% (trough) was commenced in Malmö, Sweden in 1958 Lovqvist, et al J Intern Med 1997;241:395-400
IMPACT OF AGE OF INITIATION AND DOSING OF PROPHYLAXIS ON JOINT OUTCOME (Petrini P: Amer J Ped Hematol/Oncol 1991;13:280-7)
Evolution of Hemophilia Treatment First 3 cases of AIDS in hemophilia patients 1982 Life expectancy 10 1900 Concentrate available 1970’s 2005 1900 1964 Cryo-precipitate discovered 1974: NIH Consensus conference on non-A, non-B hepatitis
Evolution of Hemophilia Treatment Opportunistic infection described in patient with hemophilia 1982 Dr. Nilsson’s report of prophylaxis benefit 1992 NHF endorses prophylaxis 1996 First gene therapy trial initiated 1999 2005 1980 1985 Products heat treated for viral inactivation 1992 rFVIII licensed in US 1996 Dr. Marilyn Manco-Johnson’s RCT initiated
Study to Prevent Joint Damage in Young Children with SevereFactor VIII Deficiency PI: Marilyn Manco-JohnsonUniversity of Colorado at Denver and Health Sciences Center and The Children’s Hospital With the JOS Investigators: T. Abshire S. Bleak D. Brown G. Buchanan A. Cohen D. DiMichele M. Hacker W.K. Hoots C. Leissinger P. Mathew A. Matsunaga D. Medeiros D. Nugent M. Recht B. Riske A. Shapiro G.Thomas A. Thompson L. Valentino
Study Objective • To evaluate structural joint outcome in young children with hemophilia A treated with regular replacement infusions of factor VIII (prophylaxis) compared with an enhanced episode-based regimen.
Hypotheses • Primary: • Prophylaxis will be associated with less joint damage • Secondary: • Limitations of Prophylaxis therapy may be: • adherence, cost, stress, difficulty with venous access • Limitations of Enhanced Episode-basedtherapy may be: • bleed-related morbidity and life-threatening bleeding
Study Design • Prospective, Multi-center, Randomized, ControlledClinical Trial • (Approved by IRBs: CDC, COMIRB, local sites) • Radiologists reading primary endpoint were blinded to subject arm and bleeding history • Eligibility • F VIII < 2% • Age 6 - 30 months • Negative history for an inhibitory FVIII antibody • < 2 Hemorrhage/Index Joint (Ankles, Knees, Elbows)
Primary Outcome: Preservation of bone & cartilage in 6 index joints (ankles, knees, elbows) at age 6 years Joint Failure: Bone or cartilage damage: subchondral cysts, erosions or narrowed joint space
Study Schema • Recruit • Screen for Eligibility • Obtain Informed Consent Randomize ProphylaxisrFVIII 25 U/kg qod Enhanced Episodic No routine infusions Treatment of Acute Joint Bleed 40 U/kg immediately 20 U/kg at 24 & 72 hours 20 U/kg qod until complete resolution of pain and normal physical exam, up to 4 weeks Exit: Joint Outcome on MRI & X-Ray at Age 6 Yrs
Adherence with Protocol Infusion Adherence was excellent: 86% in Prophylaxis and 95% in Enhanced Episodic Data Completeness was excellent: 85 - 94% of data elements
Primary OutcomeProportion of Children with No Failure by MRI Among the Six Index Joints at Exit Compared with Prophylaxis,RR for Joint Damageon Enhanced Episodic = 6.29 (CI 1.6-26.6) using MRI outcome Prophylaxis → 84% relativerisk reduction MRI and XR: 86% agreement Episodic – 58% Prophylaxis – 93% 0% 20% 40% 60% 80% 100%
Secondary Outcomes by Treatment Arm • Annual Bleeding Events • Joint (lower, darker) • Other (upper, lighter) Annual Joint Physical Exam Scores Prophylaxis ArmEnhanced Episodic Arm
VIII Consumption in IU/kg/yr by Treatment Arm Prophylaxis Arm Enhanced Episodic Arm
MRI and Bleeding Correlation N = 346 Joints r = .36 R2 = 0.13 MRI Showed Modest Correlation with # of Hemarthroses Joint Failure Corresponds to MRI Score 7-10
Subclinical Hemarthroses Can Resultin Chronic Joint Disease % Children with Joint Failure # of Joint Hemorrhages Prior to Determination of Failure
Conclusions • Joint outcome was better in children on prophylaxis than on enhanced episodic therapy. • In children on episodic therapy, the number of joint hemorrhages did not reliably predict structural joint outcome on MRI. Future studies should include both structural as well as clinical bleeding outcomes. 3. Abnormal MRI outcome in joints with no or little bleeding suggests that the pathophysiology of joint damage is more complex than number of clinical hemorrhages and may be related to chronic subclinical leakage of blood into joints.
Conclusions 4. Despite the surprising evidence for joint damage following minimal documented bleeding on the episodic arm, after 5 years of follow-up, joints with 1 to 5 hemarthroses on prophylaxis did not show joint damage. 5. Most families (93%) were able to adhere to the demands of prophylaxis; however joint failures in two children on the prophylaxis arm were both caused by failures in adherence.
Acknowledgements Parents and Participants CDCGrant #U27/CCU812106 Special Thanks to Bruce Evatt,Mike Soucie, Lisa Richardson, Harland Austin and Sally Crudder. Hemophilia & Thrombosis Research Society (HTRS) NIH CRCGrant #R00069 FACTOR DONATION: Bayer HealthCare(17,000,000 Units of Kogenate (FS))Special thanks to Dick Lutes, Peter Larsen and Eduard Gorina Study Coordinators Core Team:Sharon Funk Sheryl Giambartolomei Michele Hacker David Ingram Pam Isaacs Linda Jacobson Ray Kilcoyne James Murphy Rachelle Nuss Judy Primeaux Rick Shearer Laurie Shroyer DSMB: Lou Aledort Mary Jo Cleaveland Gary Cutter Sue Havens Dave Tubergan Mark Yarborough
Barriers to Prophylaxis: • Cost ($3,000-6,000/kg/yr) • Time/effort of every other day home venipuncture • Stress of treating an unwilling child • Central Venous Access Device: Use/Complications • Adherence with long-term therapies • (Hacker et al, Haemophilia 2003)
Venous access devices are surgically implanted reservoirs that drain into major veins.
Complications of CVADs: infection (0.3/1000 days) thrombosis (50% at 4 years) mechanical dysfunction
Self-infusion of factor concentrates can be taught to children as young as 6 years.
Where we are now… • Recombinant molecules have improved safety and availability for replacement therapy for hemophilia. • Recombinant technology is the basis for gene therapy. • Home infusion offers excellent prevention, but is expensive, complicated, stressful.
Where we are going… • “Designer Molecules” made by tailored mutations in FVIII and FIX provides the opportunity to improve upon Mother Nature for persons with hemophilia
Recombinant Production: The Human FVIII Gene (1) Is Inserted Into A Vector With A Promoter (2) And Carried Into CHO Cells Where It Directs FVIII Synthesis (3).
How can FVIII be improved for manufacture, replacement therapy or gene therapy? • ↑ Synthesis • ↑ Release • ↑ Activity • Inactivation ↑ Plasma circulation
How the cell makes protein Nucleus:mRNA copied from DNA Ribosomes:proteins are built ER:protein processing (folding, add carbohydrates, SO4, PO4, bridging) Golgi:protein packaging, secretion
The Structure of Human Factor VIII gene and protein are known Upper panel: post-translational modifications: fully, partially, non and potentially glycosylated asparagine, disulfide bridges, free cysteine, and sulfated tyrosine. Lower panel: Intracellular and extracellular cleavages. Mannucci, Tuddenham N Engl J Med 2001;344:1773-9.
Improved Production: Increased Gene Expression (mRNA) Translate the gene into more copies of proteins BDD FVIII ↑ mRNa 20x but ↑ secretion 2x Substitute FVIII introns 1 & 13 with truncated FIX intron 1 ↑ secretion 13x Future: How can VFIII Be Improved? Designer FVIII
FVIII with 6 Glycosylation Sites from the B-Domain has Increased Expression and Secretion. Miao, et al, Blood 2004;103:3412-19. A little bit of the Beta Chain improves secretion by binding to LMAN1
FVIII Production Can Be Improved By Designer Mutations in the B-Domain FVIII expression in cell culture is improved with Refacto BDD and 5-times more with 226/N (FVIII activity by 1-stage, white bars, Chromogenic Black bars) The short B-Domain spacer also increases secretion by improved ER Transport by LMAN1.
Reduce ER Chaperone Protein Interactions • Chaperone protein, BiP • Resides in the ER • Binds and degrades improperly folded FVIII • Consumes energy (ATP) • Holds back FVIII transfer • A single point mutation • Phe309 Ala BiP Binding • 3x ↑ FVIII Secretion
3-D view of FVIII on cell surface A point mutation in the A1 Domain (Phe309Ser) improves secretion efficiency Factor VIII molecules on Liposomes Stoilova-McPhie, et al. Blood 2002;99:1215-23.
Increased Activation by Thrombin Asp 713-Arg 740 of FVIII is replaced by Ile51-Leu80 of Heparin Cofactor II & more readily activated (Voorberg, et al. J Biol Chem 1996;271:20985-88.)
FVIII Resistance to Inactivation IR8: Arg 740 Ala; 794-1689 deleted 5-fold Specific activity (Pipe, et al. Proc Natl Acad Sci 1997;94:11851-6).Cysteine substitutions at 664 & 1826 Disulfide bond (Gale, et al. JTH 2003;1:OC094



![Sales Forecast for Recombinate Market [Hemophilia A and B]](https://cdn4.slideserve.com/1425739/recombinate-hemophilia-a-and-b-forecast-and-market-analysis-to-2022-by-globaldata-dt.jpg)