Download

1 / 52
540 likes | 738 Views
N u t r i t i o n a n d l i v e r c i r r h o s i s. 萬芳醫院營養室 江詩雯 2005.03.03.

E N D
Nutritionandlivercirrhosis 萬芳醫院營養室 江詩雯 2005.03.03
Influence of the metabolic complications of liver cirrhosis on dietary intakeNurdan TMed Sci Monit 2000; 6 :1223-1226Nutritional therapy in cirrhosisGiulio M, Rebecca M, Federica A and Giampaolo BJ Gast Hepa 2004; 19 :S401-405Post-feeding hyperammonaemia in patients with transjugular intrahepatic portosystemic shunt and liver cirrhosis: role of small intestine ammonia release and route of nutrition administrationPlauth M, Roske AE, Romaniuk P, Roth E, Ziebig R and Lochs HGut 2000; 46 :849-855
Fatty liver www.gicare.com/ pated/gifs/elv0004.gif www.gutfeelings.com/ CRLIVER.JPG
Normal healthy liver, surface is smooth and uniform Sever cirrhosis, surface is very nodular www.gihealth.com/ newsletter/34/two_livers.jpg
pain nausea vomiting anorexia constipation Wt loss fatigue nutrition metabolism hypoglycemia ascites anemia portal pressure splenomegaly leukopenia venous pressure thrombocytopenia bleeding edema EV erectile dysfunction menstrual disorders hormone metabolism jaundice bilirubinemia bilirubin metabolism intestinal bile Vit. K absorption total liver failure clay-colored stool urobilingen dark urine HE coma death liver inflammation liver necrosis
Complications of liver cirrhosis • Portal hypertension • Esophageal varices (EV) • Ascites • Hyperammonaemia • Hepatic encephalopathy (HE) • Hepatorenal syndrome
Malnutrition is an early and typical aspect of hepatic cirrhosis. • 70% of p’t with cirrhosis have signs of PT/Cal malnutrition. Lautz et al. 1992 Crawford et al. 1994 Prijatmoko et al. 1993
Way to lead malnutrition • food intake (anorexia, nausea, drugs) • malabsorption • energy and PT requirement • paracenthesis induced PT loss • complications
Malnutrition • mortality (35% v.s. 16% in normal-fed p’t) • complications : ascites (44% v.s. 24%) Lautz et al. 1992
p’t with advanced liver disease should be recommended a diet providing adequate calories, proteins, minerals and vitamines. • Dietary supplementation is much essential in CLD, which can decrease malnutrition,infections and sepsis happened. Nompleggi and Bonkovsky 1994
p’t with cirrhosis can be observed early postprandial hyperinsulinemia, which results in early satiety and decrease hunger via cholecystokinin (CCK). • It directly actions on the brain. Richardson et al. 1994
Nutrition in the complications of liver cirrhosis • Calories (Cal) • Fat • Protein (PT) • Carbohydrate (CHO) • Sodium (Na) • Fluid • Vitamins
m. • Total Cal=REE*1.2 or 30 kcal/kg • Fat=30-35% of total Cal • PT=1g/kg/d HE :10-20g/d (3-5d 5-10g) ESPEN Consensus group : req. 1-1.5g/kg/d low PT diet may worsen HE • CHO=remainder of the Cal requirement Plauth et al. 1997 Nurdan 2000
HE • Vegetable PT : 1. intraluminal pH 2. ammonia secretion 3. transit time • suggest 30-40g/d Nurdan 2000
Na : not exceed 2g(88mmol)/d • Daily sodium intake : 130 (mmol/kg) * wt change (kg/d) + 24h urinary Na (mmol/d) – 10 (mmol/d) • Tense ascites : 40mmol/d • Na free diet : energy, PT, lean body mass • Na intake should be restricted before fluid
Way to lead Na depletion • NSAID • Vasopression analogues • Large volume paracentesis without volume expansion • Diuretic therapy
Fluid : no need to restrict at the beginning • Vitamins : supplement water and fat solutable vit.(B1, B12, folate, A, D, E, K)
Alb.: (1)p’t don’t receive alb. had significantly more distrubances in electrocyte, PRA and creatinine level than those who received it. no difference in survival (2)iv. filtered to ascitic fluid and doesn’t remain in the intravascular compartment. Furthermore cause alb. degeneration and be harmful in PT deficiency states.
iv BCAAs in cirrhosis with acute encephalopathy Riggio et al. 1982 Wahren et al. 1983 Michel et al. 1985 Cerra et al. 1985 Fiaccadori et al. 1985 Strauss et al. 1986 Vilstrup et al. 1990 • 7 controlled studies • BCAAs group v.s. glucose or non selective AA soln. or lipid groups • BCAAs was gave for 2-6 d • Post treatment observation period : 4-16 d • 201(BCAAs) v.s. 179(isocaloric group) • No statistically significant in survival
Certainly BCAAs don’t worsen encephalopathy and may be safely used to maintain an adequate PT intake in subjects at risk of altered mental state. • BCAAs may be easily used as energy sources, thus improving nitrogen balance and have a beneficial on anorexia. Plauth et al. 1997 Panella et al. 1987 Tessair et al. 1996 Laviano et al. 1997 Davidson et al. 1999
Oral BCAAs in cirrhosis with or without chronic encephalopathy • Oral BCAAs are generally used in athletes • 9 controlled studies • BCAAs (7-30g), alcoholic cirrhosis (29-90%), latent encephalopathy (0-79%), lactulose (8-100%) • BCAAs supplementation can only be recommended in p’t at high risk of encephalopathy Eriksson et al. 1982 Sieg et al. 1983 Simko et al. 1983 McGhee et al. 1983 Horst et al. 1984 Guarnieri et al. 1984 Christie et al. 1985 Fiaccadori et al. 1988 Marchesini et al. 1990
A multicenter, randomized study, > 1 yr, 174 p’t • (a) BCAA supplementation group • (b) maltodextrins group (equicaloric) • (c) lactoalbumin group (equicaloric/nitrogenous) Non-BCAA group
Long term BCAA supplementation increases survival time and prevents to decrease hospital admission rates.
BCAA-enriched formulations can be useful in p’t who are intolerant to PT and malnourished, which can improve PT synthesis and reduce post injury catabolism. Nompleggi and Bonkovsky 1994
BCAA-enriched soln. increased serum alb. also reduced morbidity and improved the quality of life. • BCAAs strongly activate mTOR signaling in liver, which is the cellular nutrition sensor for PT translation initiation. Poon et al, 2004 Nishitani et al, 2004
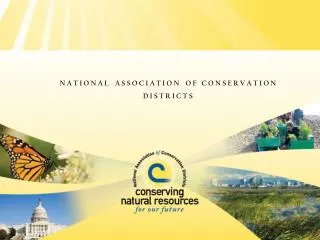
Transjugular Intrahepatic Portosystemic Shunt (TIPS) Hepatic vein Expandable stent Portal vein www.med-ars.it/ galleries/gastro16.htm
Liver cirrhosis, ascites, hepatorenal syndrome Small intestine mucosa extracts glutamine from arterial blood for metabolism of enterocytes and releases ammonia into portal vein TIPS hyperammonaemia Hepatic encephalopathy
Methods • Enteral AA infusion (TIPS : 5/8) • Parenteral AA infusion (TIPS : 3/8) • ND tube (2mL/kg/h) • Drugs: tobramycin 80mg, colistin 100mg, amphotericin B 500mg qid to reduce ammonia production from intestinal bacterial
Ammoniagenic AA : Glycine & Gln. CHO:182g/L Fat:56g/L NaCl:170mmol/L Gln. : 274 μmol/kg/h Provide Cal substrates and maintain hormonal response, mucosal perfusion comparable
Enteral or parenteral AA infusion Infusion over -10 -5 0 15 30 60 90 120 180 240 min Blood was sampled in triplicant and then centrifugated and deproteinisated/ Analysis for ammonia and Gln.
Methods • Arterial blood • Superior mesenteric venous (SMV) blood • Data are given as mean (SEM) • Values were calculated as area under the curve of venous-arterial differences • Two tailed t test • SPSS and Excel • P <0.05
EN ammonia Gln. 157 60 74
PN ammonia Gln. 115
ammonia Gln.
166 107 65 85 62 50 ammonia SMV-artery Gln. SMV-artery
ammonia Gln. EN PN EN PN
ammonia Gln.
Results • Small intestine is a source of post-feeding hyperammonaemia in liver cirrhosis. • EN is associated with higher degree of systemic hyperammonaemia than isonitrogenous PN in cirrhosis and TIPS p’t.
Discussion • TIPS can be used to control variceal haemorrhage or ascites, but aslo associated with an increased risk of HE. Ochs et al, 1995 Nolte et al,1998 Somberg et al, 1994 Jalan et al, 1997
None of p’t had worsening of their mental state when feeding a substantial nitrogen load of 40.5g of AA/ 75kg BW within 120 min. • PT test meals in cirrhosis Staedt et al, 1993
Gln. 5.9g (14.5% of total AA) as moreammoniagenic than other AA and capable of inducing HE. • Gln. as a potentially essential PN in malnourished cirrhotic p’t deserves further clarification.
Conclusion • Gln. metabolism of small intestine is a source of increased portal ammonia concentrations and that post-feeding hyperammonaemia is caused. • PN feeding should be regarded as superior to EN in cirrhotic p’t.
Rossi-Fanelli F, Riggio O, Cangiano C, Cascino A, De Conciliis D, Merli M, Stortoni M, Giunchi G. Branched-chain amino acids vs lactulose in the treatment of hepatic coma: a controlled study. Dig Dis Sci 1982; 27:929-35 • Wahren J, Denis J, Desurmont P, Eriksson LS, Escoffier JM, Gauthier AP, Hagenfeldt L, Michel H, Opolon P, Paris JC, Veyrac M. Is intravenous administration of branched chain amino acids effective in the treatment of hepatic encephalopathy? A multicenter study. Hepatology 1983; 3:475-80 • Michel H, Bories P, Aubin JP, Pomier-Layrargues G, Bauret P, Bellet-Herman H. Treatment of acute hepatic encephalopathy in cirrhotics with a branched-chain amino acids enriched versus a conventional amino acids mixture. A controlled study of 70 patients. Liver 1985; 5:282-9 • Cerra FB, Cheung NK, Fischer JE, Kaplowitz N, Schiff ER, Dienstag JL, Bower RH, Mabry CD, Leevy CM, Kiernan T. Disease-specific amino acid infusion (F080) in hepatic encephalopathy: a prospective, randomized, double-blind, controlled trial. J Parenter Enteral Nutr 1985; 9:288-95 • Vilstrup H, Gluud C, Hardt F, Kristensen M, Kohler O, Melgaard B, Dejgaard A, Hansen BA, Krintel JJ, Schutten HJ, et al. Branched chain enriched amino acid versus glucose treatment of hepatic encephalopathy. A double-blind study of 65 patients with cirrhosis. J Hepatol 1990;10:291-6 • Eriksson LS, Persson A, Wahren J. Branched-chain amino acids in the treatment of chronic hepatic encephalopathy. Gut 1982; 23:801-6 • Sieg A, Walker S, Czygan P, Gartner U, Lanzinger-Rossnagel G, Stiehl A, Kommerell B. Branched-chain amino acid-enriched elemental diet in patients with cirrhosis of the liver. A double blind crossover trial. Z Gastroenterol 1983; 21:644-50
McGhee A, Henderson JM, Millikan WJ Jr, Bleier JC, Vogel R, Kassouny M, Rudman D. Comparison of the effects of Hepatic-Aid and a Casein modular diet on encephalopathy, plasma amino acids, and nitrogen balance in cirrhotic patients. Ann Surg 1983;197:288-93 • Horst D, Grace ND, Conn HO, Schiff E, Schenker S, Viteri A, Law D, Atterbury CE. Comparison of dietary protein with an oral, branched chain-enriched amino acid supplement in chronic portal-systemic encephalopathy: a randomized controlled trial. Hepatology 1984; 4:279-87 • Guarnieri GF, Toigo G, Situlin R, Faccini L, Rustia R, Dardi F. Muscle cathepsin D activity, and RNA, DNA and protein content in maintenance hemodialysis patients. Adv Exp Med Biol 1984; 167:533-43 • Christie ML, Sack DM, Pomposelli J, Horst D. Enriched branched-chain amino acid formula versus a casein-based supplement in the treatment of cirrhosis. J Parenter Enteral Nutr 1985 ; 9:671-8 • Marchesini G, Dioguardi FS, Bianchi GP, Zoli M, Bellati G, Roffi L, Martines D, Abbiati R. Long-term oral branched-chain amino acid treatment in chronic hepatic encephalopathy. A randomized double-blind casein-controlled trial. The Italian Multicenter Study Group.J Hepatol 1990; 11:92-101 • Nompleggi DJ, Bonkovsky HL. Nutritional supplementation in chronic liver disease: an analytical review. Hepatology 1994; 19:518-33 • Lautz HU, Selberg O, Korber J, Burger M, Muller MJ. Forms of malnutrition in patients with liver cirrhosis. Gastroenterology 1992; 70:178-86 • Plauth M, Merli M, Kondrup J, Ferenci P, Weimann A ans Muller MJ. ESPEN guidelines for nutrition in liver disease and trasplantation. Clin Nuti 1997; 16:43-55
Crawford DH, Shepherd RW, Halliday JW, Cooksley GW, Golding SD, Cheng WS, Powell LW. Body composition in nonalcoholic cirrhosis: the effect of disease etiology and severity on nutritional compartments. Gastroenterology 1994; 106:1611-7 • Prijatmoko D, Strauss BJ, Lambert JR, Sievert W, Stroud DB, Wahlqvist ML, Katz B, Colman J, Jones P, Korman MG. Early detection of protein depletion in alcoholic cirrhosis: role of body composition analysis. Gastroenterology 1993;105:1839-45 • Tessari P, Zanetti M, Barazzoni R, Biolo G, Orlando R, Vettore M, Inchiostro S, Perini P, Tiengo A. Response of phenylalanine and leucine kinetics to branched chain-enriched amino acids and insulin in patients with cirrhosis. Gastroenterology 1996;111:127-37 • Laviano A, Cangiano C, Preziosa I, Riggio O, Conversano L, Cascino A, Ariemma S, Rossi Fanelli F. Plasma tryptophan levels and anorexia in liver cirrhosis. Int J Eat Disord 1997; 21:181-6 • Davidson HI, Richardson R, Sutherland D, Garden OJ. Macronutrient preference, dietary intake, and substrate oxidation among stable cirrhotic patients. Hepatology 1999; 29:1380-6 • Poon RT, Yu WC, Fan ST, Wong J. Long-term oral branched chain amino acids in patients undergoing chemoembolization for hepatocellular carcinoma: a randomized trial. Aliment Pharmacol Ther 2004; 19:779-88 • Nishitani S, Ijichi C, Takehana K, Fujitani S, Sonaka I. Pharmacological activities of branched-chain amino acids: specificity of tissue and signal transduction. Biochem Biophys Res Commun 2004; 313:387-9 • Plaitakis A, Smith J, Mandeli J, Pilot trial of branched-chain amino acids in amyotrophic lateral sclerosis. Lancet 1988; 1:1015-8 • The Italian ALS Study Group, Branched-chain amino acids and amyotrophic lateral sclerosis: a treatment failure? Neurology 1993; 43:2466-70
Child-Pugh score Interpretation:Class A: 5-6 Class B: 7-9 Class C: 10-15