Download

1 / 67
1.55k likes | 4.82k Views
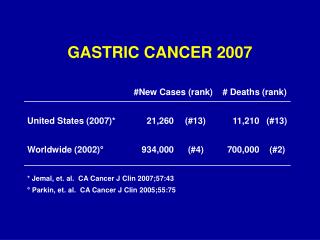
Gastric cancer. The department of Gastroenterology Shanghai Ren-Ji Hospital Zhi Hua Ran ( 冉志华 ). Epidemiology . Second most common cancer related death. Forth common types of cancer. (2000). (2000). Gastric Cancer . Geographic variations (ten times). Continuing decline.

E N D
Gastric cancer The department of Gastroenterology Shanghai Ren-Ji Hospital Zhi Hua Ran (冉志华)
Epidemiology Second most common cancer related death Forth common types of cancer (2000) (2000) Gastric Cancer Geographic variations (ten times) Continuing decline Primarily a decline of distal GC
Geographic distribution of mortality rates for gastric cancer in males in China
Etiological Factors of Gastric Cancer H. pylori Genetic factors Gastric Cancer Environmental factors Precancerous changes
The role of H. Pylori infection in gastric carcinogensis Epidemiological studies RF: 2.8~6 folds Type I carcinogen 1994 by IARC Attributable risk 50%~73% Animal modes (Mongolian gerbil) Gastric Cancer Honda et al . 1998 Watanabe et al. 1998
Environmental factors Japanese immigrants in US: 25% Second generation: >50% Subsequent generations: comparable to General US population Environmental factors are involved
Environmental factors Lower socioeconomic status Mucosal damage Poor food storage Fresh vegetable/fruits /Micronutrition Pro-carcinogen/ Carcinogen GC Tobacco/alcohol Lack of antioxidant Eating salted/ Smoked food
Genetic factors The majority of gastric tumor are sporadic in nature There are rare inherited gastric cancer predisposition traits such as germline p53 (Li-Fraumeni syndrome) E-cadherin (CDH1) alterations in diffuse gastric cancers
Precancerous changes Precancerous lesions Precancerous conditions
Precancerous lesions Defined as those pathological changes predisposed to gastric cancer dysplasia 10% of patients may progress in severity majority of patients either regress or remain stable High-grade dysplasia may be only a transient phase in the progression to gastric cancer occurs in atrophic gastritis or intestinal metaplasia
Nature history of gastric dysplasia 5 years 5 years 10% No Dysplasia Mild Dysplasia Moderate Dysplasia 60% 60% 5 years 10% 3 months-2 years 10% Gastric adenocarcinoma 50%-90% High-grade Dysplasia
Precancerous condition Defined as those clinical setting with higher risk of developing gastric cancer Chronic atrophic gastritis Gastrectomy Pernicious anemia Menetrier’s disease Chronic gastric ulcer Gastric polyps
Postulated sequence of histologic events in the progression to gastric adenocarcinoma and potential contributory factors Correa hypothesis H. Pylori Other factors FAP or Adenomas Other factors Chronic Superficial Gastritis Gastric Adenocarcinoma Intestinal Metaplasia Atrophic Gastritis Dysplasia Association Strong Association
Pathology Stages Morphology Pathohistologic classification Metastasis
Stages Early stage limited in the mucosa and submucosa layers, no matter with or without lymph node metastasis Classified by the Japanese Society for Gastric Cancer <1cm <0.5cm Advanced stage invaded over submucosa According to Bormann’ classification
TNM classification (UICC) 0 Tis N0 M0 III AT2 N2 M0 I AT1 N0 M0 T3 N1 M0 I BT1 N1 M0 T4 N0 M0 T2 N0 M0 III BT3 N2 M0 II T1 N2 M0 IV T4 N2 M0 T2 N1 M0 T1~3 N3 M0 T3 N0 M0 any T any N M1
Pathohistologic classification Histology Adenocarcinoma 90% Lymphoma 5% Stromal 2% Carcinoid <1% Metastasis <1% Adenosquamous/squamous <1% Miscellaneous <1%
Origin (Lauren) Intestinal type associated with most environmental risk factors carries a better prognosis shows no familial history Diffuse type consists of scattered cell clusters with poor prognosis
Growth pattern (Ming) Expanding type grew en mass and by expansion resulting in the formation of discrete tumor nodules with relatively good prognosis Infiltrative type invaded individually with poor prognosis
Metastasis Direct invasion Lymph node dissemination Blood spread Intraperitoneal colonization
Special term Blumer shelf A shelf palpable by reactal examination, due to metastatic tumor cells gravitating from an abdominal cancer and growing in the rectovesical or rectouterine pouch Krukenberg tumor A tumor in the ovary by the spread of stomach cancer
Clinical manifestation Signs and Symptoms Early Gastric Cancer Asymptomatic or silent 80% Peptic ulcer symptoms 10% Nausea or vomiting 8% Anorexia 8% Early satiety 5% Abdominal pain 2% Gastrointestinal blood loss <2% Weight loss <2% Dysphagia <1%
Signs and Symptoms Duration of symptoms Less than 3 month 40% 3-12 months 40% Longer than 12 month 20% Advanced Gastric Cancer Weight loss 60% Abdominal pain 50% Nausea or vomiting 30% Anorexia 30% Dysphagia 25% Gastrointestinal blood loss 20% Early satiety 20% Peptic ulcer symptoms 20% Abdominal mass or fullness 5% Asymptomatic or silent <5%
Special signs & terms Linitis plastica:diffusely infiltrating with a rigid stomach Virchow’s node:supraclavicular lymphadenopathy (left) Irish’s node:axillary lymphadenopathy Sister Mary Joseph’s node:umbilical lymphadenopathy
Laboratory tests Iron deficiency anemia Fecal occult blood test (FOBT) Tumor markers (CEA, Ca19-9)
Diagnosis Endoscopic diagnosis --- biopsy needed for definitive diagnosis Radiologic diagnosis Detection of early gastric cancer
Endoscopic diagnosis In patients with signs and symptoms suggestive of GC, and/or with compatible risk factors or paraneoplastic conditions, the diagnostic procedure of choice could be an endoscopic examination The diagnostic criteria for early or advanced gastric cancer under endoscopy are based on the JRSGC and Bormann’s classification
Radiologic diagnosis For reasons of cost and availability, radiography may sometimes be the first diagnostic procedure performed Classic radiography signs of malignant gastric ulcer asymmetric/distorted ulcer crater ulcer on the irregular mass irregular/distorted mucosal folds adjacent mucosa with obliterated /distorted area gastricae nodularity, mass effect, or loss of distensibility
Radiologic diagnosis Proximal GC Linitis plastica Distal GC
Detection of early gastric cancer Endoscopic screening general population or high risk persons Careful observation Japan is the only country that had conducted large nationwide mass population screening of asymptomatic individuals for gastric malignancy
Differential diagnosis Gastric Cancer Gastric Ulcer
Complications GI bleeding 5% Pylorus/cardia obstruction Perforation ulcer type
Treatment Surgical resection EMR Adjuvant therapy Palliative therapy
Endoscopic mucosal resection Gastric cancer lesion confined to mucosa layer Endoscopic ultrasound (EUS) is helpful in stageing GC
Chemotherapy Adjuvant chemotherapy may increase 5 years survival rates and decrease the relapse rates Combination chemotherapy are recommended
Tumor Cell Kinetics Non-proliferative cells G2 2h 1~2h M S Death 2~30h G0 hs~ds G1 Temporally non-dividing cells (souse of tumor recurrence) Proliferating cells (tumor growth)
Classification of anti-tumor agents • Traditional classification • Classification based on cell kinitics
Traditional classification Alkylating agents(烷化剂): They counteract cancerous cell division by cross-linking the two DNA strands in the double helix so that they cannot separate. Such as chlorambucil(苯丁酸氮芥), cyclophosphamide,(环磷酰胺) ,thiotepa(塞替派), and busulfan (白消安). Alkylating agent
Traditional classification Antimetabolites(抗代谢类): They replace natural substances as building blocks in DNA molecules, thereby altering the function of enzymes required for cell metabolism and protein synthesis. Including: purine antagonists (巯基嘌呤、磺硫嘌呤钠、6-硫鸟嘌呤) pyrimidine antagonists (5-氟尿嘧啶、阿糖胞苷、5-氟尿嘧啶脱氧核苷) folate antagonists (甲氨碟呤)
Traditional classification Antitumor antibiotic(抗癌抗生素):They act by binding with DNA and preventing RNA (ribonucleic acid) synthesis, a key step in the creation of proteins, which are necessary for cell survival. Doxorubicin (柔红霉素) Mitomycine (丝裂霉素) Bleomycin (博莱霉素)
Traditional classification Plant alkaloids(植物碱):They are antitumor agents derived from plants. These drugs act specifically by blocking the ability of a cancer cell to divide and become two cells. Although they act throughout the cell cycle, some are more effective during the S- and M- phases, making these drugs cell cycle specific. Vinblastine: 长春花碱 Vincristine: 长春新碱 Taxol: 紫杉醇 Irinotecan (CPT-11): 依立替康 Camptothecin: 喜树碱 Hydroxycamptothecin:羟基喜树碱 Elemene: 榄香烯乳