Download
1 / 41
420 likes | 856 Views
Gastric Cancer, Pancreatic Cancer, and Hepatobiliary Cancers. Objectives. The learner will be able to: Identify the various risk factors, signs, and symptoms for specific types of gastrointestinal cancers.

E N D
Gastric Cancer, Pancreatic Cancer, and Hepatobiliary Cancers
Objectives The learner will be able to: • Identify the various risk factors, signs, and symptoms for specific types of gastrointestinal cancers. • Discuss care implications related to treatment for specific types of gastrointestinal cancers.
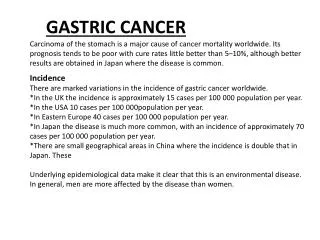
Gastric Cancer (Stomach Cancer) • American Cancer Society (ACS) estimates for 2012: • 21,320 new cases of stomach cancer • 10,540 deaths from stomach cancer • Almost 2 out of 3 people found to have stomach cancer are older than age 65. • Slightly higher risk in men • Common throughout the world, much less common in the United States • Reasons may have to do with food storage and less use of salted and smoked foods. • May be because of the use of antibiotics to treat infections; these drugs can kill H. pylori, which may be a major cause of stomach cancer.
Gastric Cancer: Risk Factors • Infection with Helicobacter pylori (H. pylori) • Age: Sharp increase after age 50 • Gender: More common in men • Ethnicity: More common in Latinos and African Americans than in Caucasians, and most common in Asian/Pacific Islanders • Where a person lives: High rates of stomach cancer in Japan • Diet: Increased risk with diets high in smoked foods, salted fish and meats, and pickled vegetables • Smoking doubles the risk. • Type A blood • Certain cancer syndromes • Family history of stomach cancer • Type of work: Workers in coal, metal, and rubber industries seem to have an increased risk.
Gastric Cancer: Signs and Symptoms • Anorexia • Unintended weight loss • Abdominal pain • Vague discomfort in the abdomen, often above the navel • A sense of fullness just below the sternum after eating a small meal • Heartburn, indigestion, or ulcer-type symptoms • Nausea • Vomiting with or without blood • Ascites
Gastric Cancer: Diagnosis • Upper endoscopy • Biopsy • Upper GI series • Endoscopic ultrasound • CT scan +/- needle biopsy • MRI • PET scan • Laparoscopy • Labs (CBC, chemistries, LFTs)
Gastric Cancer: Treatment • Surgery • Unresectability criteria include advanced locoregional disease, distant metastasis, or peritoneal seeding. • Chemotherapy and targeted therapy • Chemoradiotherapy pre- and/or postoperatively, or for metastatic or locally advanced disease • Without radiation pre- and/or postoperatively, or for metastatic or locally advanced disease • Radiation therapy • Chemoradiotherapy as above • Palliative control of symptoms
Pancreatic Cancer • Tumors of the pancreas: • Most common are exocrine tumors; nearly all of these are adenocarcinomas. • Endocrine tumors are much less common. They are know as islet cell tumors or neuroendocrine tumors. • ACS estimates for 2012: • 49,920 new cases of pancreatic cancer • 37,390 deaths from pancreatic cancer
Pancreatic Cancer: Risk Factors • Age: Risk increases with age, with almost 90% of patients > age 55. • Race: Risk higher in African Americans • Smoking: Risk 23 times higher in smokers • Obesity and lack of exercise • Diabetes • Chronic pancreatitis • Cirrhosis of the liver • Work exposure: Heavy exposure to certain pesticides, dyes, and chemicals may increase risk. • Family history • Gene mutations • Stomach problems: Too much stomach acid or H. pylori
Pancreatic Cancer: Signs and Symptoms • Pain in the abdomen or in the middle of the back • Unexplained weight loss • Jaundice • Pale, bulky, or greasy stools due to blockage of pancreatic enzymes • Nausea, vomiting, and pain that worsens after eating • Swollen gallbladder • Blood clots • Fatty tissue changes • Diabetes
Pancreatic Cancer: Diagnosis • History and physical exam • CT scan with guided needle biopsy • MRI • PET scan or PET/CT scan • Ultrasound • ERCP (endoscopic retrograde cholangiopancreatography) • Angiography • Blood tests (CBC, chemistries, LFTs) • Tumor markers: CA 19-9 and CEA • Biopsy
Pancreatic Cancer: Treatment • Surgery: Curative resections • Whipple procedure (pancreatoduodenectomy) • Distal pancreatectomy • Radiation therapy • Neoadjuvant for resectable/borderline resectable • As chemoradiotherapy for unresectable or locally advanced disease • Adjuvant postoperative therapy with chemoradiotherapy • Palliative • Chemotherapy and targeted therapy • Systemic chemo and targeted therapy is used in the neoadjuvant or adjuvant setting and in the management of locally advanced unresectable and metastatic disease.
Pancreatic Cancer: Palliative and Supportive Care • Formal palliative medicine service evaluation when appropriate • For biliary or gastric outlet obstruction: • Stenting • Bypass procedures • J-tube or PEG tube • Pain • Celiac plexus neurolysis • Palliative chemoradiotherapy • Pancreatic insufficiency • Pancreatic enzyme replacement • Thromboembolic disease • Low molecular weight heparin (LMWH)
Hepatobiliary Cancer • Hepatobiliary cancer • Hepatocellular carcinoma (HCC) • Biliary tract cancers • Intrahepatic cholangiocarcinomas • Extrahepaticcholangiocarcinomas • Gallbladder cancer • ACS estimates for 2012: • 28,720 new cases of primary liver cancer and bile duct cancer • 20,550 deaths from these cancers
HCC: Risk Factors • Chronic viral hepatitis • Heavy alcohol use • Cirrhosis • Inherited metabolic diseases • Diabetes • Obesity • Aflatoxins • Vinyl chloride and thorium dioxide (Thorotrast) • Anabolic steroids • Arsenic
HCC: Signs and Symptoms • Unexplained weight loss • Anorexia • Feeling full after a small meal • Nausea or vomiting • Fever • Hepatomegaly • Splenomegaly • Ascites • Pruritis • Jaundice
HCC: Diagnosis • History and physical exam • Ultrasound • CT scan • MRI • Angiography • Laparoscopy • Lab tests: AFP (alpha-fetoprotein) may be elevated in liver cancer and LFTs.
HCC: Staging • Several staging systems are used for liver cancer. • Following initial workup, patients are stratified into four categories: • Potential resectable or transplantable, operable by performance status or comorbidity • Unresectable disease • Inoperable by performance status or comorbidity with local disease only • Metastatic disease
HCC: Prognosis • Patients with early-stage liver cancer treated with liver transplant have a five-year survival rate in the range of 60%70%. • Patients with early-stage liver cancer that can be completely resected have a five-year survival rate of over 50%. • Patients with unresectable disease have a five-year survival rate of 10%.
HCC: Treatment • Surgery • Hepatic resection • Transplantation • Ablative procedures • Radiofrequency ablation (RFA) • Percutaneous ethanol injection (PEI) • Transarterial chemoembolization (TACE) • Transarterialradioembolization (TARE) • Systemic targeted therapy with sorafenib
Bile Duct Cancer(Cholangiocarcinoma) • 2,0003,000 people in the United States develop bile duct cancer each year. • Much more common in Asia and the Middle East, mostly because of a common parasitic infection of the bile duct • Average age at time of diagnosis is 73 years. • Two out of three people with bile duct cancer are older than age 65 when diagnosed.
Bile Duct Cancer: Risk Factors • Certain diseases of the liver or bile ducts • Primary sclerosing cholangitis • Ulcerative colitis • Bile duct stones • Choledochal cysts • Cirrhosis of the liver • Other abnormalities of the bile ducts • Liver fluke infections • Age • Obesity • Family history
Bile Duct Cancer: Signs and Symptoms • Jaundice • Itching • Light colored stools/dark urine • Abdominal pain • Anorexia/weight loss • Fever • Nausea/vomiting
Bile Duct Cancer: Diagnosis • History and physical exam • Labs: CBC, chems, LFTs, tumor markers CEA, CA 19-9 • Ultrasound • Endoscopic or laparoscopic • CT scan • CT-guided biopsy • MRI • PET scan • Cholangiography • ERCP (endoscopic retrograde cholangiopancreatography) • MRCP (magnetic resonance cholangiography) • PTCP (percutaneous transhepatic cholangiography) • Angiography • Laparoscopy • Cholangioscopy
Bile Duct Cancer: Treatment • Surgery • Biliary drainage by ERCP or percutaneous approach with stent placement • Chemotherapy • Fluoropyrimidines (5-fluorouracil, capecitabine) • Gemcitabine • Cisplatin • Chemoradiotherapy
Gallbladder Cancer • ACS estimates 6,000 new cases of gallbladder cancer in 2012. • More common in women • Incidence increases with age, with most cases being diagnosed in the seventh decade.
Gallbladder Cancer: Risk Factors • Gallstones • Porcelain gallbladder • Female sex • Obesity • Older age • Ethnicity and geography • Choledochal cysts • Abnormalities of the bile ducts • Gallbladder polyps • Typhoid
Gallbladder Cancer: Signs and Symptoms • Abdominal pain • Nausea and vomiting • Jaundice • Gallbladder enlargement • Less common: • Anorexia • Weight loss • Abdominal swelling • Severe itching • Black, tarry stools
Gallbladder Cancer: Diagnosis • History and physical exam • Labs: CBC, chems, LFTs, tumor markers CEA, CA 19-9 • Ultrasound • Endoscopic or laparoscopic • CT scan • CT-guided biopsy • MRI • PET scan • Cholangiography • ERCP (endoscopic retrograde cholangiopancreatography) • MRCP (magnetic resonance cholangiography) • PTCP (percutaneous transhepatic cholangiography) • Angiography • Laparoscopy • Cholangioscopy
Gallbladder Cancer: Treatment • Surgery • Biliary drainage by ERCP or percutaneous approach with stent placement • Chemotherapy • Fluoropyrimidines (5-fluorouracil, capecitabine) • Gemcitabine • Cisplatin • Chemoradiotherapy
Common Symptoms of Upper GI Cancers • Anorexia • Weight loss • Nausea and vomiting • Fatigue • Pain
Toxicities/Complications of Chemotherapy • GI: Nausea, vomiting, mucositis, anorexia, and diarrhea may occur. • Myelosuppression • Neurotoxicity, both acute and chronic, with oxaliplatin • Chronic neurotoxicity with cisplatin and the taxanes • Hand-foot syndrome with infusional 5-FU and capecitabine • Hypersensitivity can occur with oxaliplatin later in therapy (dose #7 or later).
Nursing Interventions • Myelosuppression: Growth factors, education on prevention of infection • GI: • Nausea/vomiting: Administer antiemetics, assess efficacy; dietary education; fluids • Mucositis: Assess oral cavity, advise on oral care protocol. • Diarrhea: Education on how to use antidiarrheal agents, fluids, low-residue diet • Peripheral neuropathy • Education and support to preserve patient safety
Conclusions • Gastric cancer, pancreatic cancer, and hepatobiliary cancers can cause debilitating symptoms. • Nursing interventions can alleviate many of these symptoms, leading to a better quality of life for patients.
References Adams, L.A., Cunningham, R.S., & Belansky, H. (2009). Anorexia. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 2536).Pittsburgh, PA: Oncology Nursing Society. Aiello-Laws, L.B., Ameringer, S.W., & Eaton, L.H. (2009). Pain. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 215234).Pittsburgh, PA: Oncology Nursing Society. American Cancer Society. (2012a). Bile duct (cholangiocarcinoma) cancer. Retrieved from http://www.cancer.org/Cancer/BileDuctCancer/DetailedGuide/index American Cancer Society. (2012b). Gallbladder cancer. Retrieved from http://www.cancer.org/Cancer/GallbladderCancer/DetailedGuide/index American Cancer Society. (2012c). Liver cancer overview. Retrieved from http://www.cancer.org/Cancer/LiverCancer/OverviewGuide/index American Cancer Society. (2012d). Pancreatic cancer overview. Retrieved from http://www.cancer.org/Cancer/PancreaticCancer/OverviewGuide/index American Cancer Society. (2012e). Stomach cancer overview. Retrieved from http://www.cancer.org/Cancer/StomachCancer/OverviewGuide/index American Joint Committee on Cancer. (2010). AJCC cancer staging handbook (7th ed.). New York, NY: Springer.
References (cont.) Eaton, L.H., & Tipton, J.M. (Eds.). (2009). Putting evidence into practice: Improving oncology patient outcomes. Pittsburgh, PA: Oncology Nursing Society. Friend, P.J., Johnston, M.P., & Eaton, L.H. (2009). Chemotherapy-induced nausea and vomiting. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 63-83). Pittsburgh, PA: Oncology Nursing Society. Griffen-Sobel, J.P. (Ed.). (2007). Gastrointestinal cancers. Pittsburgh, PA: Oncology Nursing Society. Harris, D.J., Eilers, J.G., & Eaton, L.H. (2009). Mucositis. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 193213).Pittsburgh, PA: Oncology Nursing Society. Mitchell, S.A., Beck, S.L., & Eaton, L.E. (2009). Fatigue. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 149174). Pittsburgh, PA: Oncology Nursing Society. Muehlbauer, P., Thorpe, D., & Belansky, H. (2009). Diarrhea. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 119134). Pittsburgh, PA: Oncology Nursing Society. National Comprehensive Cancer Network. (2012a). NCCN Clinical Practice Guidelines in Oncology: Gastric cancer [v.2.2012]. Retrieved from http://www.nccn.org/professionals/physician_gls/pdf/gastric.pdf
References (cont.) National Comprehensive Cancer Network. (2012b). NCCN Clinical Practice Guidelines in Oncology: Hepatobiliary cancers [v.2.2012]. Retrieved from http://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf National Comprehensive Cancer Network. (2012c). NCCN Clinical Practice Guidelines in Oncology: Pancreatic adenocarcinoma [v.2.2012]. Retrieved from http://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf Samuel-O’Garro, L., & Suozzo, S.H. (2007). Symptom management in gastrointestinal cancers. In J. Griffen-Sobel (Ed.), Gastrointestinal cancers (pp. 7588). Pittsburgh, PA: Oncology Nursing Society. Shields, S. (2011). Characteristics of cytotoxic agents. In M. Polovich, J.M. Whitford, & M. Olsen (Eds.), Chemotherapy and biotherapy guidelines and recommendations for practice (3rd ed., pp. 3855). Pittsburgh, PA: Oncology Nursing Society. Steinberg, M. (2011). Characteristics of targeted therapies. In M. Polovich, J.M. Whitford, & M. Olsen (Eds.), Chemotherapy and biotherapy guidelines and recommendations for practice (3rd ed., pp. 6272). Pittsburgh, PA: Oncology Nursing Society. Zitella, L., Gobel, B.H., & O’Leary, C. (2009). Prevention of infection. In L.H. Eaton & J.M. Tipton (Eds.), Putting evidence into practice: Improving oncology patient outcomes (pp. 267283). Pittsburgh, PA: Oncology Nursing Society.