Download
1 / 13
130 likes | 449 Views
Ogdensburg, New York. Fredric Remington Art Museum. Claxton-Hepburn Medical Center. Ogdensburg-Prescott International Bridge USA to Canada. . Claxton-Hepburn Medical Center(CHMC). 159-bed hospital; largest hospital in the largest geographic county in New York StateAnnual budget $85 million approx 18,000 ED visits/yr approx 450 deliveries/yrTertiary care facilities over 125 miles away.

E N D
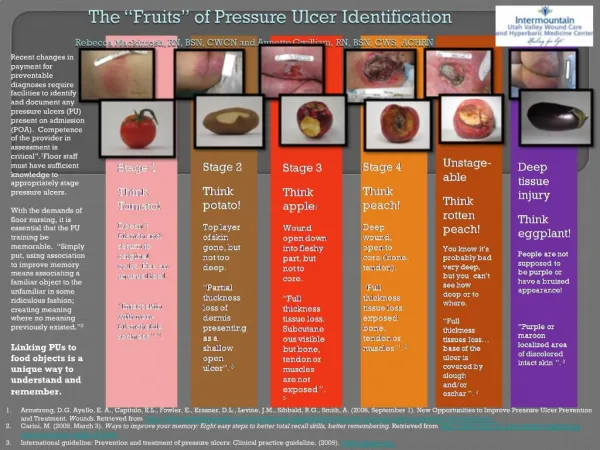
1. Perfecting Pressure Ulcer Care:
Working towards zero
Karen Cole, RN, BSN, CWOCN, CDE
Jennifer Shaver, RN, BSN, NM/ ICU
Claxton-Hepburn Medical Center
Ogdensburg, NY 13669
2. Ogdensburg, New York
3. Claxton-Hepburn Medical Center
(CHMC)
4. ICU Pressure Ulcer Prevention Program
(PUPP)
In 2003 � 2004 concerns arose over
pressure ulcer prevalence in ICU ranging
from 33% - 50%
We developed and implemented practice
changes; quickly and easily!
Introduced onto Medical Surgical Units and
our hospital-based skilled nursing facility
5. How�.
Complete skin assessment, with Braden score, documented on admission and every shift
Escalating intervention according to assessment (pressure relief, turn assist, off-loading, etc)
Included in interdisciplinary needs assessment, addressed at team meetings
Education and training on a �no-lift� policy, with purchase of appropriate equipment (pursued and received grant funding for)
6. Spring 2005
Staff confusion: What does it all mean????
�VAP, BSRCLI, RRT, IHI, 100K, PUPP � (etc)
TMI (too much information) !
ICU Performance Improvement Team sought to demystify the clinical initiatives being implemented, as well as focus on intent (positive patient outcomes)
7.
Developed �The ICU Promise�; modified to include ALL of our ongoing initiatives
Posted in ICU, and all staff welcome to sign on: 94% did!
* Received a small token of appreciation when
signed on: author-signed critical care handbook
* Handwritten thank you notes, personalized and
signed by PIT members, CEO, ICU Med Director,
VP PCS
8. ICU� and I care!
The ICU Promise
Prevents pressure ulcers, peptic ulcer disease, and deep vein thrombosis
Raises the head of the bed
Oral care is done; thoroughly and frequently
Manages pain
Includes the patient and their family in education and decision making
Sedates and weans ventilator patients appropriately
Evaluates and treats blood glucose values
Sepsis is managed, and prevented
To provide excellent care, to every patient and family, everyday!
9.
When it all came together�
64 yo fe with a BMI of 98% for AMI, complicated by CHF, Pneumonia
* Intubated on admission. Trach on day 7, ventilated for 5.5
weeks
2 minor staff injuries first hour of admission
Implemented Vent Bundle, Pressure Ulcer Prevention Program, and Glycemic Management
Staff RNs empowered to obtain appropriate bariatric equipment, including lift-free devices
Strong administrative support received for patient and staff safety
11.
Staying on target�
Educate, educate, educate!
* Implications of CMS regulations, 10/08
* Annual nursing skills fair for professional and
non-professional staff on staging and interventions;
captured �what�s working/what�s not working� at each
session
* Pressure ulcer staging cards at physician dictation
areas
12.
Staying on target�
Tracking and sharing the data
* Inclusion in organizational Strategic Plan
* Hospital-wide prevalence and incidence surveys
* ICU Scoreboard; includes documentation metrics
* Documentation and practice supporting purchase
and use of special equipment
* Electronic notification trigger to WOCN and
Dietician of pre-existing PU
Updated and reorganized �Skin Care Team�
*Uncovered �hidden players� with identification of
ED wait times as potential challenge
13.
Staying on target�
Capturing teachable moments
* �Time wounds all heels�
Avoiding complacency/encouraging ownership
*The power of anecdotes: sharing �the story�,
developing the new story
14.
Camden, S., Shaver, J., and Cole, K. Promoting the patient's dignity and preventing caregiver injury: caring for a morbidly obese woman with skin tears and a pressure ulcer. Bariatric Nursing and Surgical Patient Care March, 2007, Vol. 2, No. 1: 77-82.
Cole, K. & Shaver, J. Ideas for organizational policy changes to improve incidence of pressure ulcer incidence in an ICU. 4/2006. Presented at the Symposium on Advanced Wound Care and Medical Research Forum, San Antonio, TX.
Shaver, J. Promoting dignity and preventing caregiver injury. 11/2005. Presented at the National Association of Bariatric Nurses Conference, Ashville, NC.