Download
1 / 22
220 likes | 351 Views
The South Carolina Health Insurance Marketplace: Where are we and where are we headed?. May 14, 2013. David Slade, Vice President-Employee Benefits Abby Russell, Health & Wellness Consultant . Overview. Review of Market Share New players

E N D
The South Carolina Health Insurance Marketplace:Where are we and where are we headed? May 14, 2013 David Slade, Vice President-Employee BenefitsAbby Russell, Health & Wellness Consultant
Overview • Review of Market Share • New players • Health Care Reform (HCR) and how it will impact distribution of products • Pay or Play Modeling • SC Exchange run by the Feds • Wellness Trends – Population Health Management, How do you manage risk to stay in the game?
SC Commercial Enrollment – HealthLeaders-InterStudy(Carolinas Health Plan Analysis)
New Players • Consumers’ Choice Health Plan • South Carolina Health Cooperative • Aetna acquisition of Coventry • Individual health insurers who participate on SC Exchange • Hospital/Health System Products? • With larger systems and more risk sharing, will hospitals create their own products? • Now that hospitals have integrated delivery systems, will they compete with health insurers like other markets? • Will insurers’ build/acquire provider systems?
Federally Run Exchange in SC • Exchanges are supposed to be operational by 10/1/13 to offer products to individuals and small employers less than 50 employees by 1/1/14 • Small employers will need to chose one plan • Marketplace with numerous products, only place to receive federal subsidies based upon federal poverty level • Products will have narrower networks to get more competitive price points • Initial drafts of applications were 20+ pages if requesting subsidies and 8 pages without subsidy • Navigators, Application Counselors and Brokers
Federally Run Exchange in SC • Exchange will need to confirm data from IRS, INS and other governmental agencies • Advanceable tax credits to purchase coverage • With no planned expansion of Medicaid in SC, those eligible for Medicaid will not be eligible for subsidies on exchanges • DTC marketing – Retail Sales Strategy • BlueCross retail stores • Sample premium in Vermont – Family of 4 - $32K income, $45 per month for a $100 deductible, Single - $40K income, $317 per month
Changes in Individual/Small Group Markets for 2014 • Government has defined Essential Health Services • Minimum actuarial value is 60%, steps up to 90% • Non-Grandfathered Rates – Gender neutral and difference between younger and older can be no greater than 300% • Rates will no longer be calculated based on medical claims – young will subsidize old, males will subsidize females • Rate shock for non-grandfathered groups – early renewal opportunities for 12/1/13 • Taxes – Health Insurer Fee (2-3%), Reinsurance Fee ($63 per covered member), Outcomes Research ($1-2 per covered member), Exchange Fee (3.5% of premium)
Private Exchanges • Several will be available 1/1/14 • Similar plan designs to public exchanges but no federal subsidies are available • Employer can move to a defined contribution approach and allow employees to chose whatever they want • Mercer Marketplace will be available 1/1 to groups with 100 or more employees • Enrollment Portals where employees make elections for health and ancillary benefits • Technology and the integration of Benefits Administration and Payroll will become critical
Pay or Play Modeling • For groups over 50, dropping coverage and paying $2000 penalty per employee will not be a simple analysis • To be compliant, an employer has to offer a plan with at least 60% actuarial value and make sure the cost of single coverage doesn’t exceed 9.5% of the employee’s income • Burden then falls on employee to take employer coverage or be subject to a fine • Affordability test is challenging for industries like restaurants and hotels • Penalties are non-deductible and included on all employees working 30 or more hours
Pay or Play Modeling • No Medicaid expansion in SC will increase the cost of HCR for companies with lower paid employees • Employers need to understand their ACA/HCR incremental cost • May push some employers over 50 employees to self-funding – avoid Health Insurer Fees and new rating methodology • Some level funding products lessen the risk of traditional self funding – pooled stop loss, fund max. liability • Wellness/Population Health Management becomes more critical- incentives will go to 30% of premium/cost with an additional 20% spread for tobacco cessation programs • Compliance is more important than ever!!!
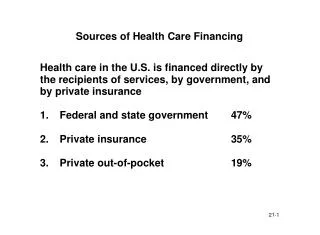
Health Care Costs Workers’ Comp Medical 22% Workers’ Comp 4% Productivity Loss 74% DIRECT Medical Care Hospitalization Pharmacy Diagnostic Testing Behavioral Health Physical Therapy Health Care Costs Lost Productivity Subpar Quality Illness & Injury Travel to Off-site MD Temporary Staffing Absenteeism Employee and Customer Dissatisfaction INDIRECT Presenteeism Turnover Replacement Training Administrative Adverse Bottom Line Impact Source: Integrated Benefits Institute, 2000 Much Better Understanding of the Total Cost of Health
Why Population Health Management? • Improve Productivity • Less absenteeism • Less sick days • Fewer medical insurance claims • Reduce utilization of prescription drugs • Increase utilization of generic prescriptions • Fewer accidents and injuries • Fewer workers’ compensation claims • Improve employee recruitment • Reduce Turnover • Improve employee morale
REACTIVE PROACTIVE Health management is now the norm, addressing a full range of needsPercent of employers offering program Addressing the continuum of health needs Source: Mercer’s 2012 National Survey of Employer Sponsored Health Plans
Population Health Continuum is Dynamic FORECASTED RISK GROUPS High Risk, Multiple Disease StatesEpisodic Case Mgmt- Inpatient Clinical Guidelines Low Risk Members Prevention and Disease Management Well & Low Risk Members Prevention Moderate Risk Members Disease Management Complex Care Inpatient - LTC
Intrinsic and Extrinsic Rewards Play an Important Role EXTRINSIC = OUTSIDE Recognition Praise INTRINSIC = INSIDE Promotions Salary Increase Feeling of Job WellDone Status Gifts Pride Sense of Achievement
Sharp growth in use of outcomes-based incentivesMore large employers linking incentives to what employees do about their health Provide incentives for achieving or maintaining health status targets Offer lower premium contributions to non-tobacco users Source: Mercer’s National Survey of Employer Sponsored Health Plans
The Flow of Health can be Affected by the Engagement Level of the Organization Program Rating Champion Comprehensive Traditional Do Nothing Rewards for Positive Actions Quality Assurance Senior Leadership Operations Leadership Self-Leadership FivePillars
Getting Started • Define Goals and Objectives • Obtain Support from Leadership • Assess Your Audience and Environment • Plan Your Program/Operating Plan • Develop Supportive Environment • Gather Data
New Trends • New Wellness Vendors Everyday • Research well – if already working with a vendor, they may be willing to work with you to meet your needs • Healthy Vending Vendors are on the rise • Be creative and use variety – may not perform HRAs annually • Healthcare Reform supports Population Health Management • Managing health becomes more critical • Incentives increase to 30% of premium with an additional 20% spread for tobacco cessation programs • Technology • Online Tools: HRAs, Health Coaching, Education Modules • Social Media provides support, accountability, and fun • Mobile Apps – resources to tracking • On-site clinics in smaller organizations • 100 or more employees approximately 4 hours or more/week • Including dependents • On-going health education coaching one-on-one if clinic is not reasonable
Our Message Your employees are one of your most important assets. We want to help ensure their health, productivity, safety, and overall well‐being. Part of that effort is to infuse wellness into your company’s culture. Our team engages clients of all sizes, providing health management program advice and implementation assistance.
Our Message Long-term goals: increased productivity, improved engagement, morale, employee retention and recruitment; decreased disability costs, health care claims, absenteeism. • Consultation helps to establish and improve health management objectives and programs in organizations of various size and industry • Together a plan design to fit your organization’s needs is developed Stewardship & Development Program Implementation Benefit Plan Design/Value Based Designed Plans • Incentive Design and Legislative consultation • On-going assistance with vendor and program coordination • Proper measurement to ensure program impact and effectiveness
Legal/regional regulatory statement to be added here if required.