Download
1 / 32
560 likes | 2.13k Views
Corynebacterium , Listeria , Erysipelothrix. Aerobic Gram-Positive Bacilli (Non-Spore-Forming). Corynebacterium : Characteristics. “ club ” “ small rod ” Gram(+), small, club shaped rod, diphtheroid Related to Mycobacterium, Nocardia – diaminopinelic acid, mycolic acid in cell wall

E N D
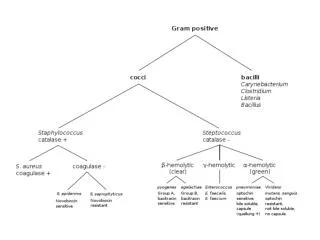
Corynebacterium, Listeria,Erysipelothrix Aerobic Gram-Positive Bacilli (Non-Spore-Forming)
Corynebacterium:Characteristics • “club”“small rod” • Gram(+), small, club shaped rod, diphtheroid • Related to Mycobacterium, Nocardia– diaminopinelic acid, mycolic acid in cell wall • Some saprophyte, plants, animals; some disease in animals, humans • Majority NF of animals, humans
Corynebacterium: Genera - Human Disease • C. diphtheriae • Toxigenic strains – diphtheria; respiratory, cutaneous • Nontoxigenic strains – pharyngitis, endocarditis • Human pathogen • C. ulcerans • Respiratory, diphtheria • Veterinary pathogen • C. jeikeium (group JK) • Septicemia, endocarditis, wound infection, foreign body (catheter, shunt, prosthesis) infection • Human skin NF • C. pseudotuberculosis • Lymphadentitis, ulcerative lyphangitis, abscess formation • Veterinary pathogen
Corynebacterium: Lab Culture • 370 C, 24 hours, pH 7.8-8.0, require oxygen • CBA – raised, translucent, gray colonies • Cystine Tellurite Blood Agar CTBA) • Enriched, selective, differential media • SRBC, bovine serum, cystine, tellurite • Tellurite inhibits RT normal flora • Corynebacterium coloniesblack, brownish due to tellurite reduction • Loeffler Coagulated Serum slant • Enriched media; serum, egg • Enhances formation metachromatic granules characteristic of Corynebacterium, visualized by methylene blue stain
C. diphtheriae: Virulence Factors - Exotoxin • Must be produced to cause diphtheria • Lysogenic bacteriophage carries "tox” gene • Trypsin cleaves toxin - fragment A (toxic activity), fragment B (tissue binding) • Toxin inhibits protein synthesis by ADP-ribosylating host cell ribosome elongation factor-2 (EF-2) • Systemic effects - heart failure, paralysis, adrenal hypofunction leading to Addison’s-like disease • C. ulcerans, C. pseudotuberculosis– some strains also make diphtheria-like toxin
Elek Plate DiphtheriaToxin Test • Immunodiffusion test in agar plate • Streak MO isolate on plate, place filter strip of antitoxin (antibody) perpendicular to streak • If MO makes toxin, at zone of equivalence (antigen + antibody) precipitate forms • Newer rapid tests: • Enzyme-linked immunosorbent assay (ELISA) • PCR DNA amplification to detect tox gene
C. diphtheriae: Virulence Factors • Capsule – protein, antiphagocytic. • Phospholipase D– dermonecrotic toxin, spreading factor • Antibiotic resistance– select for resistance during antibiotic therapy
Diphtheria: Respiratory • “leather”“skin” • MO in throats of healthy carriers • MO infects only humans, limited capacity to invade host • Disease starts as local infection of mucous membranes, causing pharyngitis • Local toxin results in degeneration epithelial cells • Inflammation, edema, pseudomembrane (fibrinclots, leukocytes, dead epithelial cells, MO) in throat
Diphtheria: Respiratory • Membrane obstructs airway, may result in suffocation • Recovery ~1 week, membrane dislodged, expectorated • Dangerous when toxin spreads systemic via blood: • heart (heart failure) • peripheral nerves (paralysis) • adrenal glands (hypofunction)
Diphtheria: Cutaneous • More common tropical, subtropical areas • Skin contact with infected person • MO colonizes skin surface, enters subcutaneous tissue through break on skin (e.g. insect bite) • Papule, chronic non-healing ulcer • Exotoxin with systemic signs
C. diphtheriae: Treatment and Prevention • Treat by giving specific antitoxin (antibody) binds and neutralizes toxin • Penicillin or erythromycin to eliminate MO, stop toxin production • DTaP vaccine - immunize withtoxoid(inactivate toxin by formalin) to elicit neutralizing antibody • Remains epidemic in developing countries due to inadequate vaccination
Other Corynebacterium: Infection and Disease • Normal flora of skin, URT • May occasionally cause disease, particularly immunocompromised • C. ulceranstoxigenic strains produce disease similar to diphtheria, , but less severe • C. jeikeium those with underlyingdisease; bacteremia, meningitis, peritonitis, wound infection • C. pseudotuberculosis those with exposure to animals (cattle, sheep, horses, goats, deer); pneumonia, lymphadenitis
Listeria monocytogenes: Characterisitcs • “blood cell” “produce” monocytosis in rabbits • G(+) short rods; singly, pairs, chains • Isolated from soil, water, vegetation, animals (bird, fish, insect) • Disease in wild, domestic animals; uncommon human infection • Facultative intracellular pathogen in humans; grows in macrophage, epithelial cells
L. Monocytogenes:Lab Culture • Aerobic, microaerophilic • Grows well on ordinary lab media • CBA – weak beta hemolysis • Able to grow slowly in cold (1°C) • Motile: • Peritrichous flagella, RT (umbrella motility) • Polar flagella, 370 C
L. monocytogenes: Lab ID • Catalase(+) • Oxidase (-) • TSI= A/A, H2S(-) • Esculin hydrolysis(+) • CAMP(+) reaction - enhanced “block” type hemolysis with Staphylococcus aureus • Grows in 6.5% NaCl • Serogroups based on O, H antigen
L. monocytogenes: Virulence Factors • Listeriolysin O (LLO) – hemolysin, pore forming toxin; escapes from phagocytic endosome to cytosol; required for intracellular growth • Phospholipase – also involve in escape of MO from endosome to cytosol • Listeric polysaccharide – capsule component
L. monocytogenes: Virulence Factors • Internalins – surface associated proteins; uptake MO into epithelial cells • ActA – surface protein; rearrangement of actin, propel MO through cell into adjacent cell (very invasive) • LPS-like substance – high fever in host • CNS Tropism - invasive
L. monocytogenes: Listeriosis • Found in environment - soil, decaying vegaetable, animal feces • Ingest contaminated animal products (milk, cheese, undercooked meat & poultry), unwashed vegetables (especially cabbage) • Disease usually mild, flu-like or GI distress • Individuals underlying chronic primary disorder • Disease - widely disseminated abscesses, granulomas; lesions may be found in liver, spleen, adrenals, respiratory tract, CNS, skin • Also meningitis with septicemia, pneumonia • High mortality may occur
Listeriosis • Uncommon disease - restricted to elderly, pregnant women, immunocompromised • Healthy children and adults – AS carriage • Pregnant moms • AS carriage, septicemia, neonatal disease • Pregnancy renders mom more susceptible (immune suppressed) • Effect on mom usually minimal, can be devastating for fetus or newborn • Immunocompromosed: • AS carriage, meningitis, septicemia, other infections
Listeriosis: Neonates • Early onset - infected transplacentally: • Septicemia, granulomatous foci in many organs • May result in abortion, stillbirth, premature delivery, death soon after birth • Baby born with cardio and respiratory distress, vomiting, diarrhea, meningitis, hepatosplenomegaly, skin lesions • Fatality rate 70-90% in untreated cases • Late onset – infected from genital tract during delivery: • Usually 1-4 weeks after birth • Manifested as meningitis • High fatality rate, but less than Early onset infection
L. monocytogenes: Treatment and Prevention • Poor prognosis in neonates • Infected moms treated as soon as disease is diagnosed to prevent transmission to fetus/neonate • Most drugs only bacteriostatic with Listeria - treatment of choice is combination penicillin and gentamycin • At risk individuals, avoid eating raw or partially cooked foods (soft cheese, turkey franks, cold cuts, vegetables)
Erysipelothrix rhusiopathiae • “red” “skin” “hair”; “red” “disease” • G(+) slender, pleomorphic, small bacilli; form filaments • Worldwide wild, domestic animals; swine main reservoir • Survives well in environment – water, soil, plant material • Animal disease widely recognized, human disease uncommon
Erysipelothrix rhusiopathiae: Lab Culture • Growth on CBA – alpha or gamma hemolysis, two types of colonies: • Smooth – rod, coccobacilli • Rough – long, thin filamentous rod • Usually 48 hours for growth • Microaerophilic, better growth in CO2 or AnO2
Erysipelothrix: Virulence Factors • Polysaccharide capsule – protect from phagocytosis • Adherence – especially heart valves • Neuraminidase – spreading • Hyaluronidase – spreading
Erysipelothrix: Clinical Significance • Primarily pathogen swine, turkey, fresh water fish • Swine - cutaneous, reddish rash; occasional complications of septicemia, endocarditis, arthritis • Humans - uncommon pathogen, zoonotic spread; erysipeloid most common form of disease
Erysipeloid • Resembles Streptococcus erysipelas skin infection • Reddish-blue, edematous lesion at site of inoculation, following trauma (abrasion, wound) to hands • Occasionally disseminates -septicemia, endocarditis, arthritis • Occupation associated disease: • Butchers - handle contaminated meat, poultry,fish animals • Farmer, veterinarian – contact with infected animals
Erysipelothrix: Treatment and Prevention • Penicillin, tetracycline, erythromycin can be used • At risk workers - should cover exposed skin when handling animals or animal products • Swine herds - should be vaccinated
Class Assignment • Textbook Reading: Chapter 16 Aerobic Gram-Positive Bacilli • Corynebacterium • Listeria • Erysipelothrix • Key Terms • Learning Assessment Questions
Case Study - Gram(+) Coccobacilli (Listeria) • A 35-year-old man was hospitalized because of headache, fever, and confusion. • He had received a kidney transplant 7 months before, after which he had been given immunosuppressive drugs to prevent organ rejection.
Case Study - Gram(+) Coccobacilli (Listeria) • CSF was collected, which revealed a white-blood cell count of 36 cells/mm3 with 96% polymorphonuclear leukocytes, a glucose concentration of 40 mg/dl, and a protein concentration of 172 mg/dl. • A Gram stain preparation of CSF was negative for organisms, but gram-positive coccobacilli grew in cultures of the blood and CSF.
Case Study - Questions • 1. What is the most likely cause of this patient’s meningitis? • 2. What are the potential sources of this organism? • 3. What virulence factors are associated with this organism? • 4. How would this disease be treated? Which antibiotics are effective in vitro?