Download
1 / 10
110 likes | 901 Views
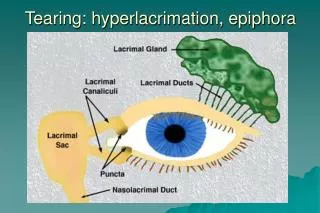
Tearing: hyperlacrimation, epiphora. Dry eye: tear break-up time, Schirmer test. Epiphora: -malpositioning -obst. INFECTIONS OF LACRIMAL PASSAGES. 1. Congenital nasolacrimal duct(NLD)obstruction. 2. Congenital dacryocele. 3. Chronic canaliculitis. 4. Dacryocystitis. Acute

E N D
INFECTIONS OF LACRIMAL PASSAGES 1. Congenital nasolacrimal duct(NLD)obstruction 2. Congenital dacryocele 3. Chronic canaliculitis 4. Dacryocystitis • Acute • Chronic
Congenital nasolacrimal duct obstruction • Caused by delayed canalization near valve of Hasner,Common • On pressure reflux of purulent material from punctum Epiphora and matting Infrequently acute dacryocystitis
Treatment of congenital nasolacrimal duct obstruction • one third: bilateral • Role out congenital glaucoma • Massage of nasolacrimal duct:10strokes 4 times a day • antibiotic drops 4 times daily: if..discharge • Improvement by age 12 months in 95% of cases • If no improvement - probe at 12 months • Results - 90% cure by first probing • 6% by repeatedprobing
Congenital dacryocele Distension of lacrimal sac by trapped amniotic fluid (amniontocele) caused by imperforate valve of Hasner • Bluish cystic swelling at or below medial canthal • tendon • May become secondarily infected • Do not mistake for encephalocele • - pulsatile swelling above medial canthal tendon Treatment • Initially massage • Probing if massage fails
Acute dacryocystitis Usually secondary to nasolacrimal duct obstruction and tear stasis • May develop into abscess • Intraosseous obstruction • Tender canthal swelling • Mild preseptal cellulitis Treatment • Systemic antibiotics and warm compresses • DCR after acute infection is controlled
Chronic dacryocystitis Epiphora and chronic or recurrent unilateral conjunctivitis Painless swelling at inner canthus Expressed mucopurulent material Treatment - DCR