Brachial P lexus
Brachial P lexus. By : Morakinyo Oyedele 1227.

Brachial P lexus
E N D
Presentation Transcript
Brachial Plexus By :MorakinyoOyedele 1227
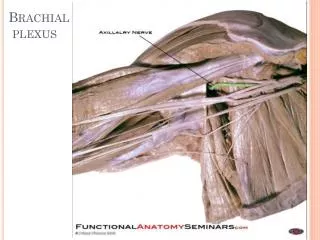
The brachial plexus is a network of nerves that conducts signals from the spinal cord, which is housed in the spinal canal of the vertebral columm (or spine), to the shoulder, arm and hand. These nerves originate in the fifth, sixth, seventh and eighth cervical (C5-C8), and first thoracic (T1) spinal nerves, and innervate the muscles and skin of the chest, shoulder, arm and hand. Brachial plexus injuries, or lesions, are caused by damage to those nerves.
Injuries to the brachial plexus affect cutaneous sensations and movements in the upper limb. They can be caused by stretching, diseases, and wounds to the lateral cervical region (posterior triangle) of the neck or the axilla. Depending on the location of the injury, the signs and symptoms can range from complete paralysis to anesthesia. Testing the patient's ability to perform movements and comparing it to their normal side is a method to assess the degree of paralysis. A common brachial plexus injury is from a hard landing where the shoulder widely separates from the neck (such as in the case of motorcycle accidents or falling from a tree). These stretches can cause ruptures to the superior portions of the brachial plexus or avulse the roots from the spinal cord. Upper brachial plexus injuries are frequent in newborns when excessive stretching of the neck occurs during delivery. Studies have shown a relationship between birth weight and brachial plexus injuries; however, the number of cesarean deliveries necessary to prevent a single injury is high at most birth weight.
For the upper brachial plexus injuries, paralysis occurs in those muscles supplied by C5 and C6 like the deltoid, biceps, brachialis, and brachioradialis. A loss of sensation in the lateral aspect of the upper limb is also common with such injuries. An inferior brachial plexus injury is far less common, but can occur when a person grasps something to break a fall or a baby's upper limb is pulled excessively during delivery. In this case, the short muscles of the hand would be affected and cause the inability to form a full fist position.
Heavy impact to the shoulder is the second common mechanism to causing injury to the brachial plexus. Depending on the severity of the impact, lesions can occur at all nerves in the brachial plexus. The location of impact also affects the severity of the injury and depending on the location the nerves of the brachial plexus may be ruptured or avulsed. Some forms of impact that affect the injury to the brachial plexus are shoulder dislocation, clavicle fractures, hyperextension of the arm and sometimes delivery at birth. During the delivery of a baby, the shoulder of the baby may graze against the pelvic bone of the mother. During this process, the brachial plexus can receive damage resulting in injury. The incidence of this happening at birth is 1 in 1000. This is very low compared to the other identified brachial plexus injuries.
Medial Cord Branches • MMMUM "Most Medical Men Use Morphine" - medial pectoral, medial cutaneous nerve of arm, medial cutaneous nerve of forearm, ulnar, medial root of the median nerve
Some mnemonics for remembering the branches: • Posterior cord branches • STAR - subscapular (upper and lower), thoracodorsal, axillary, radial • RATS- Radial nerve, Axillary nerve, Thoracodorsal nerve, Subscapular
(Upper & Lower)nerve. • ULTRA - upper subscapular, lower subscapular, thoracodorsal, radial, axillaryULNAR-Upper subscapular nerve, Lower subscapular nerve,Nerve to lattissimusdorsi, Axillary nerve, Radial nerve. • Lateral Cord Branches • LLM "Lucy Loves Me" - lateral pectoral, lateral root of the median nerve
Lateral Cord Branches • LLM "Lucy Loves Me" - lateral pectoral, lateral root of the median nerve, musculocutaneous • Love Me Latha (LML) - Lateral pectoral nerve, Musculocutaneous nerve, Lateral root of Median Nerve.
Wing scapula • In most cases of winged scapula, damage to the serratusanterior muscle causes the deformation of the back. The serratus anterior muscle attaches to the medial anterior aspect of the scapula (i.e. it attaches on the side closest to the spine and runs along the side of the scapula that faces the ribcage) and normally anchor the scapula against the rib cage. When the serratus anterior contracts, upward rotation, abduction, and weak elevation of the scapula occurs, allowing the arm to be raised above the head. The long thoracic nerve innervates the serratus anterior; therefore, damage to or impingement of this nerve can result in weakening or paralysis of the muscle.[ If this occurs, the scapula may slip away from the rib cage, giving it the wing-like appearance on the upper back. This characteristic may particularly be seen when the affected person pushes against resistance.