Download
1 / 47
490 likes | 1.47k Views
Brachial Plexopathies. William McKinley, MD Associate Professor Department of PM&R. Incidence & Prevalence. 10% of all peripheral nervous system lesions involve brachial plexus 14% of upper extremity neurological disorders due to brachial plexopathy

E N D
Brachial Plexopathies William McKinley, MD Associate Professor Department of PM&R
Incidence & Prevalence • 10% of all peripheral nervous system lesions involve brachial plexus • 14% of upper extremity neurological disorders due to brachial plexopathy • Bimodal Distribution–Obstetric: male/female 1:1, R>L–Age 20-30 y/o males 2^MVA, knife/bullet wounds - unilateral dominant limb
Etiologies • ClosedOpen–Traction Injuries Neurovascular–Radiation Gunshot Wound–Tumor (1^2^) Laceration–Surgical Positioning Surgical Trauma–Brachial Neuropathy Needles–Thoracic Outlet Syn.–Hematoma–Blunt trauma/Fx’s
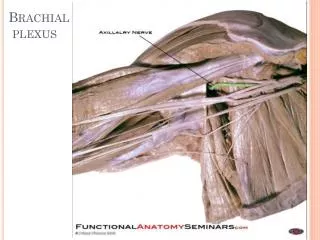
BP Anatomy • Anatomy–Ventral Rami C5-T1–Prefixed (C4) or Postfixed (T2)–RTDCB, “Palindrome” (53635)–Preganglionic vs postganglionic –Supraclavicular (roots & trunks) vs Infraclavicular (cords & branches)–cords are named (lateral, posterior, medial) by their relationship to the axillary art.–Lateral cord (C5, 6, 7), Medial cord (C8, T1), Posterior cord (C5, 6, 7, 8 & T1)
BP Injuries: Classification • Supraclavicular (roots & trunk) • Root Avulsions • Poor prognosis • affects posterior primary rami (pasaspinal m’s) • Sensory NCS potentials normal • Proximal Root Nerve Lesion–Dorsal Scapular Nerve–Long Thoracic Nerve–Suprascapular Nerve
BP Injuries (cont.) • Upper Trunk “Erb-Duchenne”–Most common BP Injury–Weakness at shoulder, EF, sensory loss C5-6 (Positioning: Add & IR)–Prognosis: Best–Causes: Trauma, Traction –Obstetrical –Brachial Neuropathy • Lower Trunk “Dejurine-Klumpe”–Clinical: Horners–Metastatic Tumor, Pancoast Tumor
BP Injuries (cont.) • Infraclavicular (Cords/Branches) • Axillary Nerve • Shoulder dislocations • Humeral neck fractures • GSW or misplaced needles • General anesthesia, neuralgic amyotrophy
BP Injuries (cont.) • Musculocutaneous Nerve • Anterior shoulder dislocation • arm extension • Weight lifting • Malpositioning • Neuralgic Amyotrophy • Radial Nerve • GSW or trauma to axilla • Improper crutch fitting
BP Injuries (cont.) • Median Nerve • Ulnar Nerve • Thoracic Outlet Syndrome (TOS) (NCS-ulnar, sensory, motor and median motor abnormalities) • Panplexopthy–Causes: Trauma, Severe Traction –Metastasis/Radiation • Prognosis: Poor
Mechanism of Injury • Traction/Stretch - trauma, positioning • Contusion/compression - trauma, tumor • Laceration - trauma, bullet, knife • Ischemia - trauma, vascular
Preganglionic vs Postganglionic • Preganglionic = prox. to “sensory” dorsal root gang. (distal to “motor” ant. horn cell) • Nerve Root Avulsion -Conn. Tissue Covers spinal nerve, traction force transferred to dura = root rupture!–Ventral roots move vulnerable - sensation often spared, motor lost–78% of BP result in some root avulsion–C8 and T1 are more susceptiple (lack c.t.) • Root avulsion = Poor prognosis! • Sensation lost... but sensory NCS is Normal • Paraspinal M’s abnormal on EMG • Positive “Axon reflex test”
Etiologies of Injury • Closed trauma - MVA (motorcycle), back pack palsy, fractures (humerus, shoulder) • Burners (“stingers”) - sports • Birth Injuries–Supraclavicular–Occurring during L&D (not forceps) • Perioperative–Etiology: traction and positioning–Primarily upper plexus–Good prognosis
Etiologies (cont.) • Violence-related–Knife, bullets (Laceration or Concussion-neuropraxia) • Primary tumors: usually benign (Schwannomas) • Metastatic tumors–Lung and breast (also lymphoma and sarcoma) • Lung (pancoast tumor - C8, T1, lymphadenopathy) •Radiation therapy –Greater than 6 but less than 24 months –Unlikely with less than 6000 R –Radiation plexopathy favors upper trunk. Mestatatic disease favors lower trunk
Neuralgic Amyotrophy • Described by Parsonage & Turner in 1948 • Characteristics: Acute onset of shoulder pain of a deep, stabbing, burning nature, aggravated by shoulder movement, muscles may be tender on exam. pain may radiate to the trapezius, arm, forearm or hand. Intense pain last up to 3 weeks and is then replaced by dull ache that may persist for months. Within 2 weeks the patients c/o weakness involving the painful limb- many associate pain subsiding as weakness begins. Muscle wasting occurs rapidly.
Neuralgic Amyotrophy • Synonyms–Brachial Neuropathy/Plexitis/Neuritis/Plexopathy–Parsonage-Turner syndrome • Incidence: 1.64 per 100,000 population • Male: 2:1 • Age of Onset: usually 20-40 years (3 mo - 74 years reported)
Antecedent or Associated Illness: Roughly 45% patients–Serum Inoculation Sickness–Typhus, Variola, Diptheria, Influenza, Triple Vaccine & Tetanus Toxiod • Weakness–Shoulder Girdle (C5, 6) - 50%–Single Peripheral Nerve - 10%•Radial LT, Axillary, SS, Phrenic
Senory Deficits: 67% –Axillary N and Lateral Antebrachial Cutaneous N • Bilateral: 33% (right 54%) • Histopathology: wallerian degeneration from axonal loss • Prognosis: Good
Natural History: Functional recovery 36% first year, 75% second year, 89% third year • Rehabilitation: no therapies effectively alter eventual outcome –Daily PROM is important to prevent contractions
Pathophysiology of BP Lesions • Neuropraxia: Conduction Block–Ischemic: short duration, recovery minute to hours–Demyelinative: physical damage to segment of myelin, necessitating remyelination. Denervation (axon loss) does not ensue; several weeks to months to recover–Good prognosis
Axonotmesis: Axonal Loss without “supporting” Structural (conn. tissue) Damage–Axon distal to injury site undergoes degeneration.–Restored function often occurs: nerve length and extent of damage are considerations to recovery
Neurotmesis: Axon Loss with supporting Structural Damage–Axon, Endoneurium, Perineurium, Epineurium destroyed.–Axons may regenerate along aberrant pathways, misdirection of motor and sensory nerves, scarring impedes nerve regrowth.–Poor prognosis
History & Physical • Expertise in anatomy and functional anatomy prerequisite! • Hx: mechanism of injury, change of sx, pain • Observation: Horners synd (ptosis, myosis), winging of scapula, atrophy, skin changes • Exam: motor, sensory, DTR, ROM, tinnels, vascular • Additional studies: EMG/NCS, Xray
Differential Diagnosis • Peripheral nerve injuries • Radiculopathies • SCI
Radiologic (and other) Studies • Electromyography • C-Spine, shoulder xrays • MRI • Myelography • Axon reflex testing–Histamine “Triple response of Bonney”–Vasodilation, wheal, flare–NL in “preganglionic (poor prog)–ABNL in “post” (better prog)
Electrodiagnostic Eval of Brachial Plexus Injury • Summary–motor and sensory potential (esp amplitude) and needle EMG (PSW, Fibs) are most sensative indicators of axonal loss–Paraspinal EMG usually normal. Abnormalities indicate preganglonic injury (radiculopathy, SCI)–SSEP, F-waves and H-reflexes (LS Plexus) may be delayed or absent b/c depend on proximal conduction
–Poor Prognosis: preganglionic, panplexopathy • Conduction Block–Drop in CMAP amplitude exceeding 20% without temporal dispersion–Failure of afferent and efferent impulse propagation across affected site–Prognosis evaluation at appx 10 days to 2 weeks
–SNAP, CMAP, NCV, EMG should be normal–Decreased recruitment may be present with increasing force production • Demyelination–Slowing of NCV 25-30%–Increased temporal dispersion
Axonal Loss–Wallerian degeneration ensues–Sensory loss evidenced by decreased amplitude or loss of potential, but preganglionic lesions, like radics, have preserved SNAP with sensory loss which has poor prognosis. 7-10 days SNAP’s disappear.
–Compound Motor Action Potential has decreased amplitude that precedes SNAP changes secondary to sensory nerve lack of NMJ, which disintegrates at 6-7 days. It is important to compare side amplitude difference. (>50% signifies axon loss)
–EMG Shows spontaneously depolarization evidenced by fibrillations and positive sharp waves that can occur at 7-10 days in muscles close to the injury and 4-6 weeks in muscles distal from lesion. Increased insertional activity and decreased recruitment also present.–NCS may be normal until late
Conservative Management • Strengthening, ROM • Sling for protection and subluxation • One-handed activities • Complicated braces ( ? usefulness) • Pain management (begin early, do not amputate, meds), stellate ganglion blocks • Edema control
Psychological counseling • Vocational support
Surgical Treatment: Generalizations • No surgery for preganglionic injuries • Surgical treatment in closed “total” (whole plexus) supraclavicular injuries • Timing: 6-12 months • Alternative: amputation plus arthrodesis plus prosthesis • C8-T1 - defer to surgical reconstruction • C5-7 - better prognosis, shoulder arthrodesis plus tendon transfer
Lumbosacral Plexopathy • Lumbar plexus L1-3(4)–Terminal nerves - femoral, obturator–Sensory loss: L1-3(4)–Weakness: hip flexors, knee extensors, hip adductors–Differentiate from femoral nerve injury (no hip adductor weakness)
Sacral plexus (L4-S2)–Terminal nerves - sciatic (tibial & peroneal), Gluteal (superior & inferior)–Differentiate from sciatic n injury (no hip abductor/extensor weakness)–May include anal sphincter muscles • Etiology: pelvic injury, retroperitoneal hematoma, neoplasm, RT, traction, idiopathic