Download
1 / 28
280 likes | 313 Views
This study explores subcortical disorders, focusing on white matter changes, disease processes, and cognitive characteristics. It covers various pathologies like Multiple Sclerosis, HIV, and Ischemic Vascular Dementia, detailing their impact on cognitive functions.

E N D
Subcortical Disorders Thomas G. Bowers, Ph.D.
Pathology Sample Kinney, Korein, Panigraphy et al. (1994)
Karen Quinland • Pathology sample indicated prominent subcortical damage • Especially in the thalamus • However, there is also evidence of considerable cortical damage • 835 grams
Anthony Bland Case • At age 18 suffered cerebral anoxia secondary to crushing injuries. • Brain weighed 1007 grams (average ~1300 grams). • Narrowed gyri, cerebral atrophy
AB Pathology Sample Jarmulowicz (1995), Catholic Medical Quarterly
Cingulate Gyrus Mamimilary Bodies Anterior Thalamus Fornix Hypothalamus Hippocampus The Circuit of Papez: An Early Model of Neural Substrates of Emotion
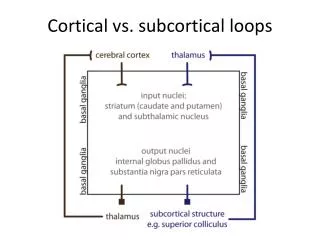
White Matter in Cognition • Three types of white matter fibers • 1. Association fibers • Connect different regions • 2. Commissural fibers • Connect corresponding hemispheres • 3. Projection fibers • Up-down
White Matter Changes in Aging • Leukoaraisosis • No mass effect, does not enhance • Periventricular sources • Glio cell loss • Small vessel infarct • Arteriosclerosis • Infection/inflammation • Demyelination • Vasculitides
MRI Characteristics • Patchy, diffuse hyperdensity • Pencil thin lines
Cognitive Characteristics • Attentional processes • Working memory (not span) • Encoding and retrieval • Spatial rotation • Discourse comprehension
Disease Processes • 1. Infection and autoimmune disorders • 2. Vasculitis • 3. Multiple sclerosis (MS) • 4. HIV • 5. Neurotoxic • 6. Gliomas
Infection and Autoimmune • Systemic lupus • 1. cognitive impairment fluctuates • 2. Can appear manic • 3. Deficits in retrieval, delayed recall • 4. Problems in cognitive speed and flexibility • Vasculitis • Inflammation of blood vessels
Multiple Sclerosis (MS) • Variable lesions in white matter and corpus callosum • Many different clinical courses • Periventricular changes • Very impaired on divided attention tasks
Multiple Sclerosis (MS) • Problems in reading comprehension, visual memory retrieval, verbal memory, motor slowing • Executive dysfunction • Negative recency effect noted • Possible loss of temporal codes • Do well on STM tasks
HIV • Patchy white matter changes • Atrophy in later stages • Prodromal stage (up to 2 years) • May be only mildly symptomatic • Attention deficits • Memory deficits • Slowed processing • Impaired conceptual processing • Impaired self monitoring
Neurotoxic Injury • Solvents • Acute and late developing effects • Headaches, dizziness, mild depression, impaired behavioral control • Problems in attention, self-monitoring • Chronic CO exposure
Gliomas • Astrocytomas (glioblastoma multiforme)
Ischemic Vascular Dementia • Leukencephalopathy • 1. Arteriosclerosis • 2. Spasm • 3. Transitant ischemia • Severity related to brain tissue loss • 1. decreased processing efficiency • 2. retrieval failures • 3. problems with semantic access • 4. spatial rotation impairment • 5. selective executive dysfunction
Progressive gliosis • Also progressive subcortical gliosis • Often may cause frontal problems
Frontal Lobe Dementia • Changes in eating habits • Sleep disturbance • Somatic complaints • Mute, empty behaviors • Not amnesic, but fail to use memory
Diffuse Axonal Injury • Acceleration/deceleration rotational forces • Yields shearing • Mechanical forces lead to neuronal segmentation, small hemorrhages, edema
Diffuse Axonal Injury • Povlishock work • Shearing due to axonal swelling, not mechanical tearing • Wallerian degeneration ensues • Evolves in 6-24 hours • Affects more distal axons • No disruption of myelin, of cell • “retraction ball” forms
Radiation Injury to Brain • Acute effects • Edema, elevated ICP • Early delayed effects, inhibition f myelin synthesis • Late delayed effects, damage to myelin, vascular damage, immune processes • Nausea, headache, drowsiness, anorexia • Verbal semantic LTM retrieval problems • Memory/motor dysfunction
Radiation Injury to Brain • Dementia can occur and lead to death • More likely memory decline, gradual recovery
Summary • White matter difficulty yields problems in complex cognitive processing • Problems in processing speed • Difficulties with high cognitive demands • Problems with complex stimulus demands, as rotations • Problems with attentional monitoring • Impairment with multiple associations
Summary • Object recognition is unimpaired, knowledge in unimpaired • No single modality of input is impaired, but multiple input is impaired