Download
1 / 70
730 likes | 1.81k Views
UNIT III:Chronic Obstructive Pulmonary Disease(COPD). INTRODUCTION.

E N D
INTRODUCTION • The most significant pulmonary diseases are those that are chronic, and these have increased dramatically in recent years. The incidence can be expected to increase annually as the number of older adults in our society increases. Because most of the diseases of the respiratory tract are not reportable to the Centers for Disease Control and Prevention, the full extent of chronic illnesses such as asthma or COPD is difficult to estimate.
Contd…. • COPD is also known as chronic obstructive lung disease (COLD) • Chronic obstructive airway disease (COAD) • Chronic airflow limitation (CAL) and • Chronic obstructive respiratory disease (CORD)
Definition : COPD is a chronic, slowly progressive disorder characterized by stable phases increasingly interrupted by worsening of symptoms termed as acute exacerbation
Contd… • It is not a disease entity but a complex of conditions that contribute to airflow limitation that is not fully reversible. • It includes emphysema and chronic bronchitis. • Most persons with COPD have one predominant disease entity, but often with manifestations of both.
Epidemiology : • Prevalence is directly related to the prevalence of tobacco smoking. • Current estimates suggest that 80 million people worldwide suffer from moderate to severe disease. • In 2005, COPD contributed to more than 3 million deaths ( 5% of deaths globally), but by 2020 it is forecast to represent the third most important cause of death world wide. • It is the 4th leading cause of mortality and 12th leading cause of disability in the united states.
Etiology and risk factors : • Cigarette smoking • Airway responsiveness and COPD • Respiratory infections • Occupational exposures • Ambient air pollution • Passive or second-hand smoking exposure • Genetic consideration • Others
1.CIGARETTE SMOKING: • Major risk factor for mortality from chronic bronchitis and emphysema. • This is in dose response relationship to the intensity of cigarette smoking which is expressed as pack years.
2.AIRWAY RESPONSIVENESS There will be increased bronchoconstriction in response to a variety of smoking related inflammation and damage results.
3. RESPIRATORY INFECTIONS • Childhood respiratory infections
4. OCCUPATIONAL EXPOSURES : • Several specific occupational exposures, including coal mining, gold mining, and cotton textile dust, have been suggested as risk factors for chronic airflow obstruction.
5. AMBIENT AIR POLLUTION : • There is increased incidence of respiratory symptoms in those living in urban compared to rural areas. • Indoor air pollution, usually associated with cooking, has been suggested as a potential contributor of COPD.
6. PASSIVE OR SECOND-HAND SMOKING EXPOSURE : • Exposure of children to maternal smoking results in significantly reduced lung growth. • In-utero tobacco smoke exposure also contributes to significant reductions in postnatal pulmonary function.
7. GENETIC CONSIDERATION : • Severe α1 antitrypsin (α1AT) deficiency is a proven early-onset genetic risk factor for COPD. • Alpha 1-antitrypsin deficiency is a genetic condition that is responsible for about 2% of cases of COPD. Alpha 1-antitrypsin protects the lungs from damage from protease enzymes such as trypsin that can be released by tobacco smoke.
8. OTHERS : • Low birth weight • Lung growth: childhood infections or maternal smoking may affect growth of lung during childhood, • Low socioeconomic status. • Nutrition .
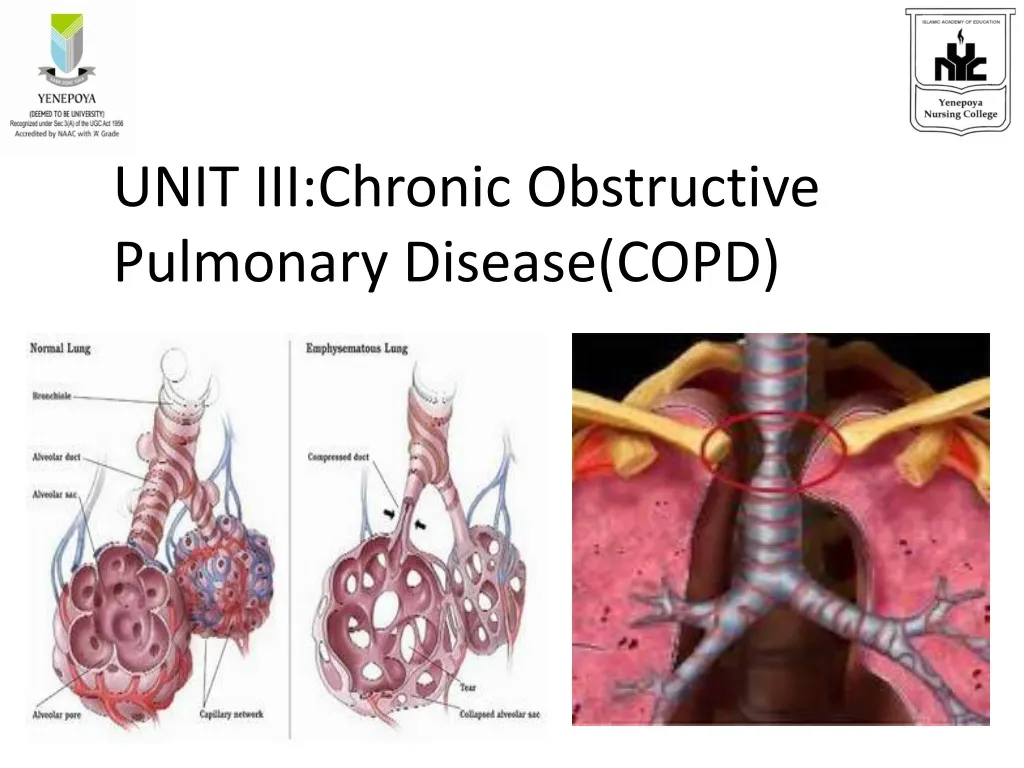
Pathophysiology: • The pathophysiologic hallmarks of COPD are : • Destruction of the lung parenchyma (characteristic of emphysema) • Inflammation of the central airways (characteristics of chronic bronchitis). • The functional consequence of these abnormalities is expiratory airflow limitation.
DEFINITION: It defined in terms of anatomic pathology as abnormal permanent enlargement of the air spaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
TYPES OF EMPHYSEMA: Depending on how the acinus is destroyed, emphysema is classified as centriacinar and panacinar. • Centriacinar emphysema: The destruction is restricted to respiratory bronchioles and central portions of the acinus surrounded by areas of grossly normal lung parenchyma. • Panacinar emphysema : The whole acinus is uniformly involved; this type is less associated with smoking and more typically occurs in alpha antitrypsin (AAT) deficient person.
PATHOPHYSIOLOGY: Connective tissue in the lungs is primarly composed of elastin, collagen and proteoglycan which can be damaged and destroyed by enzymes such as proteases and elastase.
Etiological factors such as smoking Blocks Inhibitory activity of AAT: Alveolar macrophages attracts neutrophils PMNL’s and alveolar macrophage release proteases Neutrophils release elastases Destruction of normal connective tissue – collagen, elastin structure of lung
The clinical diagnosis of the emphysema is inferred from the signs and symptoms of known pathophysiologic changes associated with the disease. • Physiologic abnormalities characteristic of emphysema include: • Increased lung compliance: • Increased airway resistance: • Altered oxygen carbondioxide exchange:
Increased lung compliance : • Loss of elastic recoil resulting from destruction of elastin in lung parenchyma causes the lungs to become permanently overdistended. • Thus compared with normal lungs, emphysematous lungs have a larger increase in volume relative to the pressure change that occurs during inhalation.
Increased airway resistance: • Destruction of elastic lung tissue causes the small airways to either collapse or narrow, particularly during expiration. • Thus air becomes trapped in the distal air spaces, contributing to the lung’s overdistended state. • The overdistended lungs press down against the diaphragm, diminishing its ventilator effectiveness.
Altered oxygen-carbondioxide exchange • Destruction of alveolar and respiratory bronchiole walls decreases alveolo-capillary membrane surface area, which inturn may diminish diffusion of oxygen and carbondioxide. • ABG remains relatively normal, although mild hypoxemia may be present. • Later , extensive surface area loss and ventilation-perfusion mismatch usually cause respiratory acidosis and hypoxemia.
CLINICAL MANIFESTATIONS : • Insidious onset of dyspnoea, initially on exertion. Later exhaling and constant dyspnoea. • Cough and sputum production. • Presence of Barrel chest. • Pursed lip breathing • “Pink puffers” • Use of accessory muscle breathing • an increased respiratory rate • a prolonged expiratory phase
DEFINITION : Chronic bronchitis is defined in clinical terms as the presence of a chronic productive cough for 3 months in each of 2 successive years in a patient whom other causes of chronic cough have been excluded.
PATHOPHYSIOLOGY : • The pathologic changes that typify chronic bronchitis are • Hypertrophy of mucus- secreting glands • Chronic inflammatory changes in the small airways.
Chronic irritation Mucus glands hypertrophy Bacteria proliferate to the lumen Excessive mucus production and impaired ciliary movement Neutrophilic chemotaxis and pus cells get in bronchial cells Peribronchial abscess leads to Airway obstruction
Obstruction of small airways Bronchospasm Atelectasis Pathologic changes move to large bronchi Increased airway resistance Diminishes surface area of respiration Ulceration and destruction of bronchial wall
Oxygen carbondioxide exchange is altered and V/Q mismatch occurs The result of these pathophysiologic alterations is hypercapnia, hypoxemia, pulmonary vasoconstriction and respiratory acidosis. Pulmonary vessel hypertension and right ventricular failure
CLINICAL FEATURES : • Productive cough, especially on awakening. • Patient appears increasingly dyspnoeic using accessory muscles to breathe. • Chronic hypoxemia result in polycythemia causes the patient to appear cyanotic. • Right-sided heart failure (cor-pulmonale) • “Blue bloaters”
Clinical manifestations : • Cough and associated sputum production are usually the first symptom, often referred to as a ‘smoker’s cough’. • Breathlessness usually brings about the first presentation to medical attention. • Edema (which may be seen for the first time during an exacerbation) and morning headaches • Modified Medical Research Council (MRC)dyspnoea scale :
Physical findings • Prolonged expiratory phase and expiratory wheezing. • Barrel chest and enlarged lung volumes with poor diaphragmatic excursion as assessed by percussion. • Patients may develop cyanosis, visible in lips and nail beds. • “Pink puffers” and “blue bloaters”. • Systemic wasting and diffuse loss of subcutaneous adipose tissue. • Hoover’s sign”.
Use of accessory muscles of respiration, • Sitting in the characteristic “tripod position” to facilitate the actions of sternocleidomastoid, scalene and intercoastal muscles.
Laboratory findings : • Pulmonary function test • Pulmonary function testing shows airflow obstruction with a reduction in FEV1 and FVC.
Chest x-ray films : • A low, flat diaphragm; increased AP diameter of the thorax; and over distension of the lungs. • Arterial blood gas analysis: • Early stage of COPD: mild or moderate hypoxemia without hypercapnia • In later stages patients have more severe hypoxemia and hypercapnia
Sputum and hematology studies: • The most frequent pathogens are S.pnuemoniae and H. influenza. • Neutrophils and bronchial epithelial cells are usually found in chronic bronchitis. • erythrocytosis is frequently seen as PaO2 levels fall below 55mmHg. • Elevated Hematocrit values
Management : • Only three interventions – smoking cessation, oxygen therapy in chronically hypoxemic patients and lung volume reduction surgery in selected patients with emphysema: have been demonstrated to influence the natural history of patients with COPD. • The main management includes : • Medical management • Surgical management • Nursing management
SMOKING CESSATION : • Advising and assisting the patient toward smoking cessation. • Complete cessation is accompanied by an improvement in lung function and deceleration in the rate fev1 decline. • In places where the indoor burning of biomass fuels is important, the introduction of non-smoking cooking devices or the use of alternative fuels should be encouraged.
















