Download
1 / 28
300 likes | 595 Views
Transient Global Amnesia. Allan B. Wolfson, MD University of Pittsburgh Department of Emergency Medicine. Presentation of TGA. Clinical features. Sudden onset Anterograde amnesia Repetitive questioning Retrograde amnesia (variable, often spotty)

E N D
Transient Global Amnesia Allan B. Wolfson, MD University of Pittsburgh Department of Emergency Medicine
Clinical features • Sudden onset • Anterograde amnesia • Repetitive questioning • Retrograde amnesia (variable, often spotty) • Normal alertness, behavior, & cognition • Non-focal neuro exam • Resolution within 24 hrs
Reported triggers • Emotional upset • Sexual activity • Vigorous exercise • Valsalva
Differential Diagnosis • Head injury • Toxic / metabolic • Vascular / TIA – posterior circulation • Non-convulsive seizure • Post-ictal state • Migraine • Tumor • Encephalitis • AV fistula • Functional
Epidemiology of TGA Age group usually over 50, but seen in kids too Family history ?2% Incidence 5 - 30 per 100,000 Recurrence 5 - 8% per year Apparent triggering factors in 33 - 50%
TGA -- Criteria for Dx • Witnessed onset • Antegrade amnesia • No clouding of consciousness or loss of personal identity • No cognitive impairment • No focal findings • No epileptic features • No recent head trauma, no sz within 2 yrs • Resolution within 24 hrs
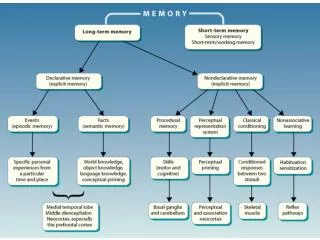
Anatomy of Memory What structures subsume memory? • Medial temporal lobes (hippocampus) • Thalamus • “Diencephalon” • Frontal / pre-frontal • “Deep cortical structures”
Physiology of Memory • Memory acquisition • Memory storage or consolidation • Memory retrieval • 3-compartment model? immediate, recent, remote
Emergency Dept Evaluation • History • Neuro exam • “Basic labs”? • Head CT • EEG • MRI
Bedside evaluation of episodic memory • Orientation? • Remember 3 things for 3 minutes? • Remember what happened yesterday?
Other types of memory to check on • Semantic memory • Procedural memory • Biographical memory • Topographic memory • Meta-memory
Etiology of TGA? • Vascular • Seizure • Migraine • Venous hypertension (Valsalva, paradoxical embolism)
Etiology of TGA? • Case-control studies show no association with stroke or TIA • Sub-group with epilepsy excluded by definition • Nonconvulsive status epilepticus? • Association with migraine • Reported precipitating factors
Differentiating features • Repetitive questioning • Complex acts and instructions • Memory gap for the event • Severity of retrograde amnesia • Rapid onset • Duration
Transient epileptic amnesia • Short attacks, multiple attacks • No repetitive questioning • Anterograde amnesia may be only partial • Altered behavior • Alteration in consciousness • Other features of epilepsy (eg, automatisms, other seizures, EEG, response to anticonvulsants)
Functional Amnesia • Severe retrograde amnesia • Absence of anterograde amnesia • Duration often weeks or longer
Fancy Diagnostic Studies • EEG • CT scanning • SPECT scanning, PET scanning • MRI, DW-MRI, PW-MRI
SPECT scanning • Some studies have shown decreased perfusion in medial temporal lobes, thalamus, or frontal lobes • Usually returns to normal after attack • Reflection of abnormality or cause?
Diffusion-weighted MRI • Inconsistent findings • Sometimes shows abnormalities (esp in left hippocampus) • Sensitive for ischemia (decreased diffusibility of water) • But also consistent with “spreading depression” (rapid resolution, unlike ischemia)
Diffusion-weighted MRI • Sensitive for ischemia (decreased diffusibility of water) • But also consistent with “spreading depression” (rapid resolution, unlike ischemia)
What is “spreading depression”? • Wave of depolarization progressing across cortex at 3-5 mm/min • Associated with aura of migraine
Diffusion-weighted MRIin TGA • Inconsistent findings • Sometimes shows abnormalities, especially in left hippocampus Bilateral or left-sided only Sometimes no changes May be time-dependent
Treatment • None necessary • Migraine therapy?
Prognosis • Essentially benign • Subclinical persistent memory deficits? • Associated conditions?
Disposition from the ED • Theoretically: after amnesia resolves, can discharge with neurology follow-up and no immediate testing • Actually: admission, MRI, EEG
Unanswered questions • Etiology? Spectrum of causes? • True role of precipitating factors? • Acute treatment? • Physiology of memory?