Download
1 / 36
370 likes | 960 Views
Atelectasis. Wilai sartcheenphong. Anatomy of lung. Background. Atelectasis From - Greek words ateles and ektasis ateles : incomplete ektasis : stretching Mean - incomplete expansion

E N D
Atelectasis Wilai sartcheenphong
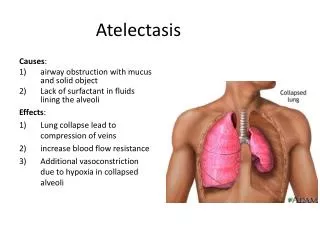
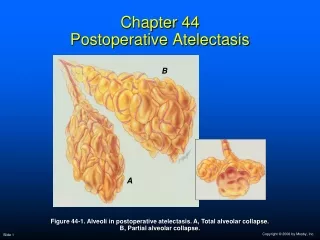
Background Atelectasis • From - Greek words ateles and ektasis ateles : incomplete ektasis : stretching • Mean - incomplete expansion - defined as diminished volume affecting all or past of a lung
Classification Divided by physiology • Obstructive atelectasis : foreign body, tumor, mucous plugging the most common type results from reabsorption of the oxygen ที่ขังอยู่ในdistal alveoli ในขณะที่มีการอุดตันระหว่าง tracheaกับalveoli โดยที่blood flow ยังปกติเกิด retraction of lungเมื่อ lung volume ลดลง ทำให้mediastinum เอียงไปด้านที่มีปอดแฟบ
Classification • Nonobstructive atelectasis 1.loss of contact between pariatal and visceral Relaxation or passive atelectasis : pleural effusion, pneumothorax 2. Compression Compression atelectasisผลจากการที่มี lesionในช่องอกแล้วทำให้ปอดด้านดังกล่าวถูกกดทับเกิดatelectasis 3. Loss of surfactant Adhesive atelectasis เกิดจากถุงลมบกพร่องในการสร้าง surfactant : ARDS
Post operative atelectasis • 20-65 % หลังผ่าตัด upper abdomen • 10 % หลังผ่าตัด Lower abdomen • หายได้เองเมื่อ Periodic deep breath, lung volumes และ flow rates กลับคืนสู่ปกติ • เป็นมากจนเกิด Hypoxemia ทำให้หายใจเหนื่อยหอบ เนื่องจาก work of breathing สูง สาเหตุเกิดจากไม่ทำ Deep breathing exercise
กลไกการเกิด (Pathogenesis) • Absent of periodic deep breath สาเหตุ Pain, general anesthetics, narcotics, splinting or bandage, abdominal distension • Decreased FRC • Retained secretion • Diaphragmatic dysfunction
อาการและอาการแสดง • หายใจตื้น • หายใจเร็ว • ทรวงอกสองข้างขยายตัวไม่เท่ากันขณะ หายใจเข้า • ฟังเสียงหายใจเบาลง • เคาะทึบข้างที่มีปอดแฟบ
Risk Factors • General risk Smoking Obesity Old age Malnutrition ASA physical status Male Uncooperative
Risk Factors • Disease-related risk Chronic respiratory disease : COPD Acute respiratory infection (upper/lower) CNS : Unconsciousness CVS : Heart failure Sepsis
Risk Factors • Surgery-related risk Operative site : upper abdomen>thoracotomy> Median sternotomy > head&neck >lower abdomen Emergency surgery Duration of surgery : > 3 hr Degree of blood loss : > 1,000 ml Resectional thoracic surgery
Risk Factors • Anesthesia-related risk Type of anesthesia : GA > RA Anesthetic management : การเลือกใช้ยา, ขนาดยา,Fluid, electrolyte Postoperative pain control Postoperative respiratory care
Preoperativepulmonaryevaluation เป้าหมาย 1. ค้นหาโรคระบบทางเดินหายใจ 2. หน้าที่การทำงานของปอดเป็นอย่างไร 3. ค้นหาปัจจัยเสี่ยง 4. พิจารณาว่าสามารถทำผ่าตัดได้หรือไม่ วิธีประเมิน 1. ซักประวัติ 2. ตรวจร่างกาย 3. ตรวจทางห้องปฏิบัติการ
hISTORY • อายุ, น้ำหนักตัว • การสูบบุหรี่ (pack/yr) • ประวัติโรคปอด/โรคที่มีผลต่อระบบหายใจ เช่น asthma, COPD, TB, sarcoidosis, neuromuscular disorder • อาการที่เกี่ยวข้องกับระบบหายใจ เช่น ไอ มีเสมหะ wheezing • การเหนื่อยหอบ (dyspnea) และ functional classification • ยาที่ได้รับ เช่น steroids, bronchodilators • ประวัติการผ่าตัดและระงับความรู้สึกที่ผ่านมา
Physical examination • Evidence of pulmonary diseases Obstructive pulmonary diseases: prolonged expiration Restrictive pulmonary diseases: rapid shallow breathing Pulmonary vascular disease: prominent 2nd heart sound, signs of right heart failure Respiratory tract infection Signs of Acute respiratory failure Ventilatory reserve :ventilatory pattern, I&E effort Sputum volume > 60 ml/day Ability to clear secretion
Physical examination • Bedside clinical tests for pulmonary function Snider ,s Match Test Forced Expiratory Time Test Breath-Holding Test Count Test Slow vital capacity Exercise tolerance
investigation • Chest X-ray (PA & lateral) • Pulmonary Function Test (PFT) Forced expiratory spirometry Maximum voluntary ventilation Respiratory muscle strength • Arterial blood gases • Electrocardiogram • การตรวจพิเศษอื่นๆ เช่น CT scan, Sputum AFB ในรายที่สงสัย
การป้องกันภาวะแทรกซ้อนทางปอดหลังผ่าตัดการป้องกันภาวะแทรกซ้อนทางปอดหลังผ่าตัด • Preoperative pulmonary preparation • Intraoperative management • Post operative respiratory care
Preoperative pulmonary preparation • Psychological preparation • ลดน้ำหนัก • Stop smoking • Good nutrition • Regular exercise • Bronchodilator therapy • Treatment of infection • Adequate mobilization of secretion • Breathing exercise and cough training
Breathing exercise • Thoracic breathing • Abdominal or diaphrag-matic breathing • Thoraco-abdominal breathing • Lateral costal breathing ผู้ป่วยCOPD ช่วงหายใจออกให้ฝึก pursed lips expirationเพื่อลด expiratory airflow obstruction ฝึกหายใจโดยใช้กล้ามเนื้อที่ไม่กระทบกระเทือนการผ่าตัด เช่น ผ่าตัด thoracotomy ให้ฝึก abdominal respiration ฝึกใช้กล้ามเนื้อเฉพาะส่วน กรณีเสี่ยงต่อปอดแฟบเฉพาะส่วน เช่น Rt. lower lobe โดยวางมือและออกแรงกดชายโครงขวา
Cough training • ไอออกทั้งหมดในคำเดียว มีประสิทธิภาพมากที่สุด แต่กระเทือนมาก เหมาะกับผ่าตัด periphery ไม่เหมาะกับผู้ป่วย COPD เกิด pneumothorax ง่าย • แบ่งไอเป็นคำสั้นๆ หลายคำ • กลั้นเป็นคำๆในช่วงหายใจออก ใช้ในผู้ป่วยที่ไม่สามารถทำ expiratory flow rate สูงพอที่จะไอ เช่น spinal cord injury
Intraoperative management • Placement of surgical incision • Minimize operation time • Minimize tissue trauma • เลือกเทคนิคระงับความรู้สึก และยาที่เหมาะสม • หลีกเลี่ยงการบาดเจ็บจากการใส่ท่อหลอดลม
Intraoperative management • ป้องกันการสำลักน้ำย่อยเข้าปอด • ขจัดเสมหะไม่ให้คั่งค้าง • ให้ยาขยายหลอดลมให้เต็มที่ • Intermittent hyperinflation • Humidified anesthetic gas • Proper fluid and blood replacement
Postoperative respiratory care • Continuation of preoperative maneuvers Lung expansion therapy : SMI therapy (Incentive spirometry) , IPPB, CPAP Promote cough • Oxygen therapy • การช่วยหายใจหลังผ่าตัด • Fowler position • Early ambulation
Postoperative respiratory care • Postoperative pain control • Gastric decompression: NG tube, treatment of ileus • Adequate nutrition • Early detection and treatment Atelectasis : relief obstruction : นอนเอาข้างที่ atelectasis ขึ้นบน : SMI therapy ดีกว่าIPPB : High CPAP : หลีกเลี่ยงการใช้ FiO2 สูง : Bronchoscopy ขจัดสิ่งอุดตัน
การบำบัดเพื่อให้ปอดขยายตัว(lung expansion therapy) • Sustained maximal inspiration (SMI) therapy มีประสิทธิภาพมากที่สุด: Incentive spirometer แนวทางปฏิบัติ 1. เลือกผู้ป่วยที่เหมาะสม:รู้ตัวดี พูดคุยรู้เรื่อง ร่วมมือ 2. สภาพปอดเอื้อ ต้องไม่หายใจตื้นหรือเร็วจนเกินไป 3. สอนการหายใจเข้าลึกสุดก่อน 4. อธิบายเป้าหมายและผลที่คาดว่าจะเกิดขึ้น 5. จัดท่าให้นั่งหัวสูง สอนเทคนิคการหายใจเข้าด้วย IS ที่ถูกต้อง ทำ 5-10 ครั้งแล้วพัก ทำทุกชั่วโมง 6. ประเมินผลการทำอย่างน้อยวันละ 2 ครั้ง 7. ประสิทธิภาพขึ้นอยู่กับเวลาที่ลูกปิงปองลอยค้างอยู่
การบำบัดเพื่อให้ปอดขยายตัว(lung expansion therapy) • Intermittent Positive pressure Breathing(IPPB) การใช้แรงดันบวกอัดก๊าซเข้าปอด ในผู้ป่วยที่หายใจเองได้ ข้อบ่งชี้ 1. ใช้ Incentive spirometer, CPAP, chest physical therapy แล้วไม่ได้ผลหรือใช้ไม่ได้(ไม่ร่วมมือ/แรงไม่พอ) 2. Aerosol delivery ในผู้ป่วยที่ไม่มีที่ไม่มีแรงหายใจเข้าลึก เช่น neuromuscular disease จัดท่า semi-Fowler หรือถ้าจำเป็นอาจให้นอนหงาย อุปกรณ์เชื่อมต่อ : facemask, mouth-piece, ETT, TT ประสิทธิภาพขึ้นกับ inspiratory volume ที่ได้
การบำบัดเพื่อให้ปอดขยายตัว(lung expansion therapy) • Continuous Positive Airway Pressure (CPAP) เพิ่ม intraalveolar pressure โดยให้ positive pressure ตลอดเวลา ทั้ง inspiratory และ expiratory phase ข้อบ่งชี้ 1. แก้ไข atelectasis ที่ไม่สามารถใช้ SMI จากการศึกษา Mask CPAP สามารถเพิ่ม FRC และลด hypoxemia in Postoperative atelectasis 2. ใช้ป้องกัน atelectasis แต่จากการศึกษาเปรียบเทียบ ในผู้ป่วยหลังผ่าตัดพบว่า CPAP ไม่ได้ดีกว่า IS or IPPB
การบำบัดเพื่อให้ปอดขยายตัว(lung expansion therapy) • Positive Expiratory Pressure (PEP) Therapy วิธีการโดยให้หายใจออกผ่านความต้านทาน ทำให้ลมหายใจออกใช้เวลานานขึ้นและความดันในทางเดินหายใจเป็นบวกนานขึ้น ป้องกันถุงลมปอดแฟบในช่วงหายใจออก เนื่องจาก alveolar distending pressure เพิ่มขึ้นในช่วงหายใจออก ช่วยให้ก๊าซเข้าถุงลมปอด โดยผ่านทาง collateral ventilation เกิดต่อเนื่องแม้ในช่วงหายใจออก ทำให้ถุงลมปอดขยายได้ดีขึ้น
การบำบัดเพื่อให้ปอดขยายตัว(lung expansion therapy) • Valsava,s Maneuver หรือ Expiratory Maneuver for Lung Expansion เป็นวิธีการที่ทำให้ปอดขยายตัวเต็มที่ โดยลดสิ่งที่อยู่ในช่องเยื่อหุ้มปอด เช่น เลือด น้ำ หรือก๊าซ ในผู้ป่วยที่ใส่ท่อระบายช่องเยื่อหุ้มปอด (Intercostal drainage) วิธีปฏิบัติ หายใจเข้าลึกเต็มที่ ทำ Valsava,s Maneuver คือ หลังหายใจเข้า ให้ปิด glottis โดยกลั้นหายใจแล้วพยายามเบ่งหายใจออกไปด้วย ค่อยๆเบ่งจนเต็มที่ ความดันในช่องเยื่อหุ้มปอดเพิ่มขึ้น ดันน้ำ ก๊าซหรือเลือดออก
สรุปการใช้lung expansion therapyทางคลินิก • ป้องกันและแก้ไข atelectasis ในผู้ป่วยกลุ่มเสี่ยง : สูงอายุ สูบบุหรี่จัด อ้วนมาก เจ็บป่วยเรื้อรัง ขาดอาหาร มีโรคหัวใจ โรคปอด มารับการผ่าตัดช่องท้องหรือทรวงอก ควรเตรียมการป้องกันตั้งแต่แรกรับหรือก่อนผ่าตัด โดยสอนให้ทำ SMI therapy, ใช้ incentive spirometer, ใช้ IPPB ให้ถูกต้อง สำหรับผู้ป่วยที่มี atelectasis แล้วต้องใช้ lung expansion therapy ร่วมกับวิธีอื่น เช่น aerosal therapy, chest physical therapy รวมทั้งหาสาเหตุและแก้ไข
References 1. ทนันชัย บุญบูรพงศ์.การบำบัดระบบหายใจในเวช ปฏิบัติ.พิมพ์ครั้งที่ 2.กรุงเทพฯ:บ้านหนังสือ โกสินทร์,2553. 2. พีรยศ ลีลารุ่งระยับ.ภาวะปอดแฟบกับกายภาพบำบัด ทรวงอก.วารสารเทคนิคการแพทย์เชียงใหม่, 29:พฤษภาคม,2539. 3.http://emedicine.medscape.com 4. http://www.healthscout.com/ency/1/440/main. 5.Robbins Pathologic Basis of Disease, 8th edition