Download
1 / 1
20 likes | 196 Views
Rhabdoid Meningioma: Case Report and Review of Literature. A mbar B. Caban Ureña 1 , Raisa Balbuena Merle 2 , Juan L. Pérez Berenger -2, , Roman Velez Rosario 2 , Juan Vigo Prieto 3

E N D
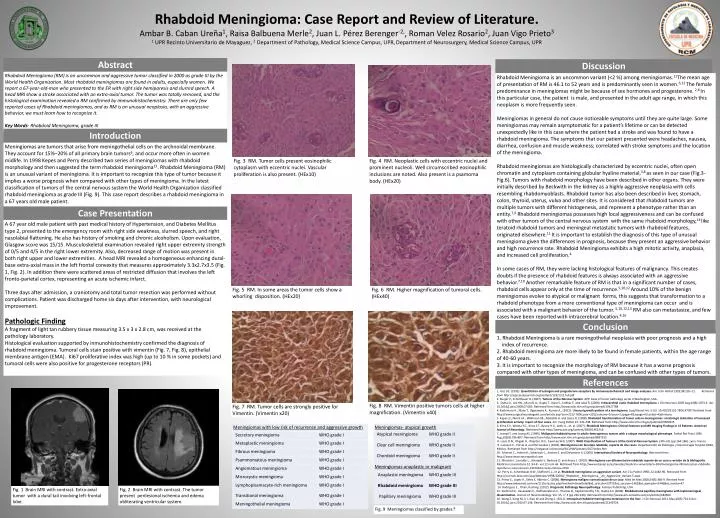
Rhabdoid Meningioma: Case Report and Review of Literature. Ambar B. Caban Ureña1, Raisa Balbuena Merle2, Juan L. Pérez Berenger-2,, Roman Velez Rosario2, Juan Vigo Prieto3 1 UPR RecintoUniversitario de Mayaguez, 2 Department of Pathology, Medical Science Campus, UPR,Department of Neurosurgery, Medical Science Campus, UPR Abstract Discussion RhabdoidMeningioma (RM) is an uncommon and aggressive tumor classified in 2000 as grade III by the World Health Organization. Most rhabdoidmeningiomas are found in adults, especially women. We report a 67-year-old-man who presented to the ER with right side hemiparesis and slurred speech. A head MRI show a stroke associated with an extra-axial tumor. The tumor was totally removed, and the histological examination revealed a RM confirmed by immunohistochemistry. There are only few reported cases of Rhabdoid meningiomas, and as RM is an unusual neoplasia, with an aggressive behavior, we must learn how to recognize it. Key Words- Rhabdoid Meningioma, grade III Rhabdoid Meningioma is an uncommon variant (<2 %) among meningiomas.11The mean age of presentation of RM is 46.1 to 52 years and is predominantly seen in women.6,12 The female predominance in meningiomas might be because of sex hormones and progesterone. 2,6 In this particular case, the patient is male, and presented in the adult age range, in which this neoplasm is more frequently seen. Meningiomas in general do not cause noticeable symptoms until they are quite large. Some meningiomas may remain asymptomatic for a patient’s lifetime or can be detected unexpectedly like in this case where the patient had a stroke and was found to have a rhabdoid meningioma. The symptoms that our patient presented were headaches, nausea, diarrhea, confusion and muscle weakness; correlated with stroke symptoms and the location of the meningioma. Rhabdoid meningiomas are histologically characterized by eccentric nuclei, often open chromatin and cytoplasm containing globular hyaline material,3,8 as seen in our case (Fig.3- Fig.6). Tumors with rhabdoid morphology have been described in other organs. They were initially described by Beckwith in the kidney as a highly aggressive neoplasia with cells resembling rhabdomyoblasts. Rhabdoid tumor has also been described in liver, stomach, colon, thyroid, uterus, vulva and other sites. It is considered that rhabdoid tumors are multiple tumors with different histogenesis, and represent a phenotype rather than an entity.7,9 Rhabdoid meningiomas possesses high local aggressiveness and can be confused with other tumors of the central nervous system with the same rhabdoid morphology,14 like teratoid rhabdoid tumors and meningeal metastatic tumors with rhabdoid features, originated elsewhere.11 It is important to establish the diagnosis of this type of unusual meningioma given the differences in prognosis, because they present an aggressive behavior and high recurrence rate. Rhabdoid Meningioma exhibits a high mitotic activity, anaplasia, and increased cell proliferation.4 In some cases of RM, they were lacking histological features of malignancy. This creates doubts if the presence of rhabdoid features is always associated with an aggressive behavior.7,10 Another remarkable feature of RM is that in a significant number of cases, rhabdoid cells appear only at the time of recurrence.5,10,12 Around 10% of the benign meningiomas evolve to atypical or malignant forms, this suggests that transformation to a rhabdoid phenotype from a more conventional type of meningioma can occur and is associated with a malignant behavior of the tumor. 5,10,12,13 RM also can metastasize, and few cases have been reported with intracerebral location.4,16 Introduction Meningiomas are tumors that arise from meningothelial cells on the archnoidal membrane. They account for 15%–20% of all primary brain tumors6, and occur more often in women midlife. In 1998 Kepes and Perry described two series of meningiomas with rhabdoid morphology and then suggested the term rhabdoid meningioma11. Rhabdoid Meningioma (RM) is an unusual variant of meningioma. It is important to recognize this type of tumor because it implies a worse prognosis when compared with other types of meningioma. In the latest classification of tumors of the central nervous system the World Health Organization classified rhabdoid meningioma as grade III (Fig. 9). This case report describes a rhabdoid meningioma in a 67 years old male patient. Fig. 3 RM. Tumor cells present eosinophilic cytoplasm with eccentric nuclei. Vascular proliferation is also present. (HEx10) Fig. 4 RM. Neoplastic cells with eccentric nuclei and prominent nucleoli. Well circumscribed eosinophilic inclusions are noted. Also present is a psamoma body. (HEx20) Case Presentation A 67 year old male patient with past medical history of Hypertension, and Diabetes Mellitus type 2, presented to the emergency room with right side weakness, slurred speech, and right nasolabial flattening. He also has history of smoking and chronic alcoholism. Upon evaluation, Glasgow score was 15/15. Musculoskeletal examination revealed right upper extremity strength of 0/5 and 4/5 in the right lower extremity. Also, decreased range of motion was present in both right upper and lower extremities. A head MRI revealed a homogeneous enhancing dural-base extra-axial mass in the left frontal convexity that measures approximately 3.3x2.7x3.5 (Fig. 1, Fig. 2). In addition there were scattered areas of restricted diffusion that involves the left fronto-parietal cortex, representing an acute ischemic infarct. Three days after admission, a craniotomy and total tumor resection was performed without complications. Patient was discharged home six days after intervention, with neurological improvement. Pathologic Finding A fragment of light tan rubbery tissue measuring 3.5 x 3 x 2.8 cm, was received at the pathology laboratory. Histological evaluation supported by inmunohistochemistry confirmed the diagnosis of rhabdoid meningioma. Tumoral cells stain positive with vimentin (Fig. 7, Fig. 8), epithelial membrane antigen (EMA). Ki67 proliferative index was high (up to 10 % in some pockets) and tumoral cells were also positive for progesterone receptors (PR). Fig. 5 RM. In some areas the tumor cells show a whorling disposition. (HEx20) Fig. 6 RM. Higher magnification of tumoral cells. (HEx40) Conclusion 1.Rhabdoid Meningioma is a rare meningothelial neoplasia with poor prognosis and a high index of recurrence. 2. Rhabdoid meningioma are more likely to be found in female patients, within the age range of 40-60 years. 3. It is important to recognize the morphology of RM because it has a worse prognosis compared with other types of meningioma, and can be confused with other types of tumors. References 1. Aziz DC. (1992). Quantitation of estrogen and progesterone receptors by immunocytochemical and image analyses.Am J ClinPathol 1992;98:105–11. Retrieved from http://ajcp.ascpjournals.org/content/123/1/21.full.pdf 2. Burger P., Schelthauer B. (2007). Tumors of the Nervous System. AFIP Atlas of tumor pathology series 4 Washington, USA. 3. Dutta D., Lee HN., Munshi A., Gupta T., Kane S., Sridhar E. and Jalali R. (2008). Intracerebral cystic rhabdoid meningioma. J Clin Neurosci.2009 Aug;16(8):1073-4. doi: 10.1016/j.jocn.2008.07.085. Retrieved form http://www.ncbi.nlm.nih.gov/pubmed/19427788 4. Kashimura H., Mase T., Ogasawara K., Kurose A., (2012). Unusual growth pattern of a meningioma. SurgNeurolInt; 3: 63. 10.4103/2152-7806.97007.Retrived from http://www.surgicalneurologyint.com/article.asp?issn=2152-7806;year=2012;volume=3;issue=1;spage=63;epage=63;aulast=Kashimura. 5. Kepes JJ., Moral LA., Wilkinson SB., Abdullah A. and Llena JF. (1998). Rhabdoid transformation of tumor cells in meningiomas: a histologic indication of increased proliferative activity: report of four cases. Am J SurgPathol 22: 231-238. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/9500225. 6. Kima E.Y., Weona Y.C., Kima S.T., Byuna H.S., Leeb J.I., et. al. (2007). Rhabdoid Meningioma: Clinical Features and MR Imaging Findings in 15 Patients. American Journal of Neurology. Retrieved from http://www.ajnr.org/content/28/8/1462.full 7. Leong FJ. and Leong AS. (1996). Malignant rhabdoid tumor in adults-heterogenous tumors with a unique morphological phenotype. Pathol Res Pract 1996 Aug;192(8):796-807. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/8897515 8. Louis D.N., Ohgaki H., Wiestler O.D., Cavenee W.K. (2007). WHO Classification of Tumours of the Central Nervous System. (4th ed). (pp.164-186). Lyon, France. 9. Luevano E., Porras A. and Hernandez J.(2002). Meningioma con fenotipo rabdoide, reporte de dos casos. Departamento de Patología y Neurocirugía hospital CIMA, México. Retrievedfrom http://conganat.uninet.edu/IIICVHAP/posters/017/index.htm 10. Mawrin C., Hahne R., Scherlach C., Kirches E. and Dietzmann K. (2004). International Society of Neuropathology. Retrieved from http://www.intsocneuropathol.com 11. Miranda I., Larralde L., Alvarado Y., Barboza O. and Ancer, J. (2010). Meningioma con diferenciación rabdoide reporte de un caso y revisión de la bibliografía. Medicina Universitaria.12 :54-8 - vol.12 núm 46. Retrieved from http://www.elsevier.es/es/revistas/medicina-universitaria-304/meningioma-diferenciacion-rabdoide-reporte-un-caso-revision-13150444-casos-clinicos-2010 12. Perry A., Scheithauer B.W., Stafford S.L., et al. Rhabdoid meningioma: an aggressive variant. Am J Su Pathol 1998; 22;1482-90. Retrieved from http://journals.lww.com/ajsp/Abstract/1998/12000/_Rhabdoid__Meningioma__An_Aggressive_Variant.5.aspx 13. Prieto S., Lopez R., Velez E, Alberto C. (2008). Meningioma maligno: comunicacion de un caso. Med IntMex 2008;24(5):366-9. Retrived from http://www.imbiomed.com.mx/1/1/articulos.php?method=showDetail&id_articulo=53771&id_seccion=1482&id_ejemplar=5446&id_revista=47 14. Rodriguez E., Tihan, Rushing. (2012). Diagnostic Pathology Neuropathology. Amirsys Publishing, USA. 15. Santhosh K., Kesavadas C., Radhakrishnan V., Thomas B., Kapilamoorthy T.R., Gupta A.K.(2008). Rhabdoid and papillary meningioma with leptomeningeal dissemination. Journal of Neuroradiology. Vol. 35, n° 4 (pp 236-239). Retrieved from http://www.em-consulte.com/en/article/184560 16. Wang Z, Kong M, Li J, Xiao W and Zheng S. (2011). Intraspinal rhabdoid meningioma metastasis to the liver. J Clin Neurosci.2011 May;18(5):714-6.doi: 10.1016/j.jocn.2010.07.146. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/21349724. Fig. 8 RM. Vimentin positive tumors cells at higher magnification. (Vimentin x40) Fig. 7 RM. Tumor cells are strongly positive for Vimentin. (Vimentinx20) Fig. 1 Brain MRI with contrast. Extra-axial tumor with a dural tail involving left-frontal lobe. Fig. 2 Brain MRI with contrast. The tumor present perilesional ischemia and edema obliterating ventricular system. Fig. 9 Meningiomas classified by grades.8