Download
1 / 49
560 likes | 896 Views
Hematology Physiology 1 Erythropoiesis. Brenda Beckett, PA-C. Hematopoiesis Erythropoiesis Pluripotent hematopoietic stem cell (PHSC) Committed stem cell (progenitor cell) Differentiation Maturation Self-renewal Proliferation. Reticulocyte Polychromasia Normocyte Erythropoietin

E N D
Hematology Physiology 1Erythropoiesis Brenda Beckett, PA-C
Hematopoiesis Erythropoiesis Pluripotent hematopoietic stem cell (PHSC) Committed stem cell (progenitor cell) Differentiation Maturation Self-renewal Proliferation Reticulocyte Polychromasia Normocyte Erythropoietin Adult hemoglobin Fetal hemoglobin Apotransferrin Transferrin Apoferritin Terms to Understand
Ferritin Hemosiderin Serum iron Total iron binding capacity -thalassemia -thalassemia Hemoglobinopathy Anemia Porphyria A,B,O,Rh blood types Terms, continued
Red Blood Cell • Transports hemoglobin • Carries oxygen from lungs to tissues • Carries CO2 back to lungs • Biconcave disc • Able to change shape • Has excess membrane
Red Blood Cell • Mature RBC has no nucleus • 5,200,000 (males), 4,700,000 (females) per cubic milliliter • Lifespan of 100-120 days • Derived from pleuripotent hematopoietic stem cells (PHSC)
PHSC • Retained in bone marrow • Reproduction controlled by growth inducers • Differentiation controlled by differentiation inducers • Will become committed stem cell (progenitor cell)
Erythropoiesis • Decreased O2 in tissues causes increased production of erythropoietin • Hormone • Formed in kidney (80-90%) and liver • Occurs in fetal liver and spleen, then shifts to fetal bone marrow • Occurs in axial skeleton and proximal end of long bones in adults
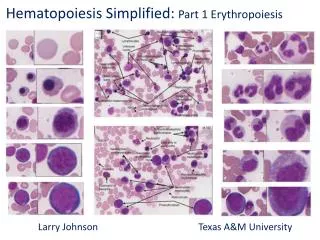
Reticulocytes • Final cell produced in marrow before release • Basophilic remnants of endoplasmic reticulum remain, becomes mature RBC (normocyte) within one day • Normally ~1% of total RBCs
Reticulocyte Count • Can differentiate between anemias due to decreased production and those of increased destruction • Will see polychromasia on Wright’s stain, need to order separate test for reticulocyte count
Hemoglobin Formation • Begins at proerythroblast stage, continues until reticulocyte (before leaving bone marrow) • Heme molecule combines with globin (long peptide chain) to form hemoglobin chain. • 4 chains bind together to form hemoglobin molecule.
Hemoglobin • Binds loosely and reversibly with O2 • Oxygen atom binds loosely with iron atom in hemoglobin • Bound as O2, released as dissolved O2
Iron Metabolism • Iron important part of hemoglobin, myoglobin and other structures • ~65% of total iron in hemoglobin • 4% myoglobin • 1% various heme compounds • 0.1% in plasma combined with transferrin • 15-30% stored in liver as ferritin
Iron Transportation & Storage • Absorbed in small intestine • Binds with apotransferrin (globulin) to form transferrin – loosely bound • Excess deposited in liver and bone marrow • In liver, combines with apoferritin to form ferritin. • Also stored as insoluble hemosiderin – iron overload
Iron Usage • If plasma iron low, iron removed from ferritin, transported as transferrin in plasma • Transferrin binds strongly with cell membranes on erythroblasts in marrow • Ingested, delivered to mitochondria • Heme synthesized
Globin chains • 4 globin chains combine with heme to make hemoglobin molecule • 95-97% of adult hgb has 2 -chains and 2 -chains (22) aka Hgb A • Fetal hgb (Hgb F) has 22. High O2 affinity, mostly changes to HgbA by birth • Hgb A2 (22), 3-5% of adult
Abnormal Hemoglobins • Hemoglobinopathies: hemoglobin chains are abnormal • Thalassemias: hemoglobin chains normal in structure but decreased or absent. Named for which chain is affected. Genes are on chromosomes 11 & 16
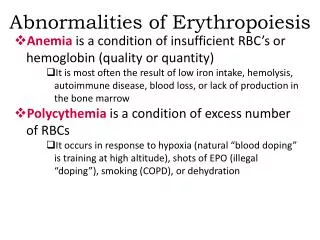
Anemia • Qualitative or quantitative deficiency of hemoglobin • Significant blood loss • Plasma replaced in 1-3 days • RBCs replaced in 3-4 weeks • Hemolysis • Deficient RBC production
Vitamin B12/Folate • Important for final maturation of RBCs • Essential to synthesize DNA • Decrease in either leads to failure of nuclear maturation and division • RBCs also become larger, irregular shape, flimsy membrane • Carry O2 normally, have short lifespan
Vitamin B12/Folate Deficiency • Macrocytic or megaloblastic anemia • Pernicious anemia: inability to absorb Vitamin B12 from GI tract • Gastric mucosa secretes Intrinsic Factor (IF), combines with B12, available for absorption • B12 stored in liver and bone marrow
Iron deficiency • When iron stores are depleted, stored iron is mobilized • When iron stores drop, hemoglobin synthesis is affected – iron deficient erythropoiesis. (hypochromic) • More severe, leads to decreased erythropoiesis, smaller cells (microcytic)
Iron Deficiency Anemia • Low iron stores = low Ferritin • Low circulating iron (transferrin) = low Serum Iron • Leads to increased Total Iron Binding Capacity (TIBC) Hypochromic, microcytic anemia
Anemia of Chronic Disease • Most likely due to inflammation • Iron stores aren’t released • Decreased erythropoiesis • Upregulation of WBC production causes decreased erythropoiesis • Normocytic or microcytic
Hemolytic anemias • RBCs are fragile, shorter lifespan • Rupture as pass through capillaries and spleen • Hereditary or acquired (immune mediated) • Increased destruction leads to increased bilirubin (jaundice)
Hemolytic anemias • Hereditary spherocytosis (and others) • Cells are spherical, can’t withstand compression – easily ruptured • Sickle cell anemia • Abnormal Hgb S (on chain) • Exposed to low O2, forms crystals, elongates cell – “sickle” • Sickle trait – protective against malaria
Thalassemias • Autosomal recessive, Mediterranean • Reduced synthesis of one globin chain, leads to microcytic anemia • or chain affected • Can coexist with hemoglobinopathies • Carrier state can be protective against malaria
G6PD Deficiency • Hereditary • Low levels of G6PD (enzyme) • Certain triggers lead to hemolysis, anemia, jaundice • Foods, medications, infection • Protective against malaria
Polycythemia • Increased number of RBCs – primary or secondary • High altitude – physiologic polycythemia • Cardiac failure, smoking, tumors • Polycythemia vera: blast cells continue to produce RBCs even though there are too many in circulation. Viscous blood. Treatment: phlebotomy
Porphyria • Inherited or acquired • Disorder of enzymes in heme pathway • 7 different types • Different combos of elevated porphyrins (heme precursors) in tissues • Excreted in urine and stool • Sx: photosensitivity, abd pain, port wine urine, muscle weakness, behavior changes
RBC/Hemoglobin destruction • Changes to plasma membranes as cell ages • Recognized by phagocytes • Phagocytosis in spleen • Heme broken down into iron & biliverdin • Biliverdin converted to bilirubin • Iron bound to transferrin
Effects of anemia • Lack of oxygen in tissues • Symptoms can be vague • Weakness, fatigue, malaise • Dyspnea • Pallor • Increased cardiac output: plapitations, heart failure
Blood Groups ABO A&B antigens: “agglutinogens” on RBC Anti-A &/or Anti-B develop in absence of antigens Will agglutinate RBCs, lyse, leads to renal failure, death
Rh Typing Other antigens can be present on RBCs Antibodies develop if exposed to antigen D (Rh), d, C, c, E, e Erythroblastosis fetalis
WBC • The overall concentration of white blood cells of all types in the blood, expressed as thousands of cells per cubic millimeter (mm3) of blood. The terms used to describe a decreased and an increased WBC are leukopenia and leukocytosis, respectively.
RBC • The concentration of erythrocytes in the blood, most commonly expressed as millions of cells per cubic millimeter (mm3). The terms describing a decreased and an increased RBC are erythrocytopenia and erythrocytosis, respectively, or, more commonly, anemia and polycythemia.
HGB/HCT • The overall concentration of hemoglobin in the blood, expressed as grams of hemoglobin per 100 milliliters of blood. • The hematocrit, the percentage of the blood volume consisting of red cells, expressed as a percent (%).
MCV • mean corpuscular volume, the average volume of individual erythrocytes in a blood sample, expressed as femtoliters (fl) per cell. One femtoliter is the equivalent of 10-15 liters. The terms used to describe an erythrocyte with a normal, decreased, or increased cell volume are normocyte, microcyte, and macrocyte, respectively.
MCHC • mean cell hemoglobin concentration, the average concentration of hemoglobin within erythrocytes, expressed as grams of hemoglobin per dL of cells. Because the intracellular hemoglobin concentration determines the density of color (suffix -chromia) of erythrocytes on a stained blood smear, the morphological descriptions associated with a normal, increased or decreased MCHC are normochromia, hyperchromia and hypochromia, respectively.
MCH • mean cell hemoglobin, the average quantity of hemoglobin in individual erythrocytes, expressed as picograms (pg) per cell. One picogram is the equivalent of 10-12 grams.
RDW • red cell distribution width, expressed as the coefficient of variation around the mean cell volume (MCV). The larger the value for RDW, the greater the variability in size within the erythrocyte population. The morphological correlate of an increased RDW is variation in the diameters of individual erythrocytes seen on the peripheral smear, or anisocytosis.
PLT/MPV • the concentration of platelets in the peripheral blood, expressed as thousands of platelets per cubic millimeter (mm3) of blood. • mean platelet volume, the average volume of individual platelets, expressed as cubic microns per platelet or as femtoliters per platelet.
RETIC • the reticulocyte percentage, or the percentage of immature erythrocytes in a peripheral blood sample. These immature cells usually constitute from 0.5 to 1.5% of the circulating red blood cell population. An absolute reticulocyte count, expressed as millions of cells per cubic millimeter (mm3), can be obtained by multiplying the RBC by the reticulocyte percentage.