Download
1 / 27
340 likes | 779 Views
Peptide Hormones. Evolving Considerations for Biotechnology and Clinical Medicine Mainstream vs. Fad Chanda Zaveri, M.S. Founder & Chairman Activor Corporation. Peptide Hormones Features & Definition. Modify protein structure and state of activity

E N D
Peptide Hormones Evolving Considerations for Biotechnology and Clinical Medicine Mainstream vs. Fad Chanda Zaveri, M.S. Founder & Chairman Activor Corporation
Peptide HormonesFeatures & Definition • Modify protein structure and state of activity • Are not metabolized by virtue of their activity • Hormone receptors – allosteric proteins • Peptide hormones – allosteric effectors
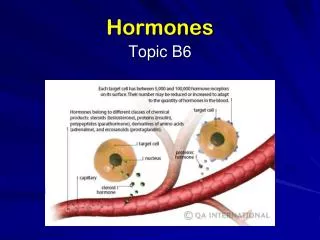
Peptide Hormone Physiology • Act on cell membrane • Act via secondary mediators • cAMP • Diacylglycerol • Calicum • Tyrosine kinase
Bioengineered Peptide Hormones • Modification of existing protein • Consider primary, secondary or tertiary structure as targets • Change in structure – new physiologic effect • Creation of novel protein
Secretagogues as Biotech Targets • Control peptide hormone synthesis and secretion • Three classes reported classically • Releasing factor hormones – GHRF • Central effectors • Hypoglycemia, dopamine, deep sleep, amino acids • Other peptide and steroid hormones • Cortisol, estrogen, thyroid hormone
HTA-5: Novel Peptide Hormone • Primary structure derived from thymic hormone, with bioengineered modifications • Physiological effect is dose dependent and cumulative • GHRF – low dose • Immunomodulation – high dose
TF-5 Literature Review • mitogenic T-cell response (Thurman, 1975) • Modulates incidence of GVHD (Fast, 1990) • Enhances NK activity of normal LGL (Serrate 1987) and tumor bearing mice (Mastino, 1992) • Increases tumor specific immunity • cytotoxic T-lymphocyte response (Zatz & Goldstein, 1983) • antigen-presenting capacity of macrophages (Tzehoval, 1989) • Stimulates proliferation of, and IL-6 production in, rat splenocytes (Attia & Badamchian 1993)
Growth Hormone vs. Age J. NIH Research April 1995
FDA Treatment Guidelines - hGH • Hypo-Pituitarism • Adult-onset Growth Hormone Deficiency
hGH SupplementationWhy are people using this? • Looking for “anti-aging” effect • Subjective Reports • Improved memory • Enhanced sexual performance • Mood elevation • More restful sleep • Enhanced exercise performance • Decrease in incidence of hot flashes
Theories of Aging • Oxidative Stress Theory • Genetic Theory of Aging • Theory of Somatopause • Hormonal Theory of Aging • Links aging to a decline in the body’s secretion of hormones WITHOUT any loss in its ability to respond to these hormones
Objective Reports bone density immune function rate of wound healing HDL, LDL in LBM, LPL blood pressure cardiac output skin thickness and hair growth General Insulin-like effect hGH Supplementation (OFF LABEL)
HTA-5 Pilot Study Profile • 15 Subjects • 7 Male & 8 Female • Age Range: 32 - 70 years • Test Duration: 6 weeks • Preparation: HTA-5 + Lysine + Arginine • Dosing: 1x daily • HTA-5: 20ng; Lys: 1200mg; Arg: 1200mg • Exclusion Criteria: [IGF-1]400ng/mL
Subjective Reports (combined study) • Improved sleep patterns • Enhanced exercise stamina • Improvement in skin texture and thickness • Decreased rate of hair loss
IGF-1 Physiology & Endpoint Considerations • Glucose Metabolism • Exerts insulin-like effect • Increases glycogen storage in SKM • Inhibits basal & insulin stimulated lipogenesis via LPL • Cholesterol Metabolism • ? Increase in hepatic cholesterol receptors • ? Suppressed synthesis • Osteoblast Metabolism • Binds to osteoblast receptor – stimulates new bone formation • IGF-2 > IGF-1
IGF-1 Response MEN WOMEN HTA-5 HTA-5 + AA
Male/Female IGF-1 Response • HTA-5 stimulates IGF-1 response • Avg IGF-1: 40.4%; > 50 years: 56.8% • Co-administration with known RFs - Synergistic IGF-1 response • DEDUCED: HTA-5 is GHRF • Generalizations • Female IGF-1 response is double that of males • IGF-1 response is age dependent • Endpoint data suggests a heightened female response
Total Cholesterol (mg/dL) 30-45 46-59 60+
Subject Cholesterol Difference Initial Final 1 231 181 -50 2 270 189 -81 3 257 241 -16 4 240 237 -3 5 241 231 -10 6 253 223 -30 7 219 209 -10 8 259 233 -26 9 239 217 -22 10 241 225 -16 11 214 203 -11 12 237 215 -22 13 218 211 -7 14 247 222 -25 15 251 239 -12 Total Cholesterol (mg/dL)
Male/Female Cholesterol Response • Avg Total Cholesterol: 23 mg/dL • Decrease in serum cholesterol • No dietary modifications • No change in medical regimen, if any • No lifestyle modifications
Bone Density (g/cm2) • Radial ultrasound • Average Increase • 6.8% HTA-5 • 12.6% HTA-5 + AA MALE FEMALE
Body Composition (kg) MEN WOMEN ATMLBM
Body Composition Response • Objective changes in TBC • Avg % ATM: 14.8% • Avg % LBM: 4.1% • Slight across age groups • Avg % body weight: 13.2% • No dietary or lifestyle modifications
Case Reports • Reversion of immuno-suppression • Cure of chronic active hepatitis B infection