Download
1 / 21
210 likes | 317 Views
HIV in Africa. What is HIV?. HIV infects primarily vital cells in the human immune system such as T cells When CD4 T cell numbers decline below a critical level, cell-mediated immunity is lost, and the body becomes progressively more susceptible to opportunistic infections.

E N D
What is HIV? • HIV infects primarily vital cells in the human immune system such as T cells • When CD4T cell numbers decline below a critical level, cell-mediated immunity is lost, and the body becomes progressively more susceptible to opportunistic infections. • Most untreated people infected with HIV-1 eventually develop AIDS. These individuals mostly die from opportunistic infections or malignancies associated with the progressive failure of the immune system. • HIV progresses to AIDS at a variable rate affected by viral, host, and environmental factors; most will progress to AIDS within 10 years of HIV infection: some will have progressed much sooner, and some will take much longer. • Treatment with anti-retrovirals increases the life expectancy of people infected with HIV. Even after HIV has progressed to diagnosable AIDS, the average survival time with antiretroviral therapy was estimated to be more than 5 years as of 2005.Without antiretroviral therapy, someone who has AIDS typically dies within a year.[
Early origins of HIV IN AFRICA • There is now conclusive evidence that HIV originated in Africa. • Astrain of Simian Immunodeficiency Virus (SIV) in a number of chimpanzee colonies in south-east Cameroon was a viral ancestor of the HIV-1 that causes AIDS in humans • Experts studying the spread of the epidemic suggest that about 2,000 people in Africa may have been infected with HIV by the 1960s
EPIDEMIC BEGINS • It was in Kinshasa in the 1970s that the first epidemic of HIV/AIDS is believed to have occurred. The emerging epidemic in the Congolese capital was signaled by a surge in opportunistic infections, such as meningitis, tuberculosis and specific forms of pneumonia. • It is speculated that HIV was brought to the city by an infected individual who travelled from Cameroon by river down into the Congo. On arrival in Kinshasa, the virus entered a wide urban sexual network and spread quickly.
HIV IN THE 1980S • Although HIV was probably carried into Eastern Africa (Uganda, Rwanda, Burundi, Tanzania and Kenya) in the 1970s, it did not reach epidemic levels in the region until the early 1980s • Throughout the 1980s it spread rapidly throughout the continent. • Truck drivers alongside other migrants such as soldiers, traders and miners - have been identified as a group which facilitated the initial rapid spread of HIV-1, as they engaged with sex workers and spread HIV outwards on the transport and trade routes. In the 1980s, 35 percent of tested Ugandan truck drivers were HIV positive as were 30 percent of military personnel from General Amin’s Ugandan army • With a few notable exceptions, the 1980s were characterized by an insufficient response to AIDS in Africa.
HIV in the 1990s • Prevalence rates skyrocketed in the 1990s
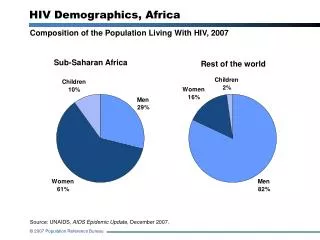
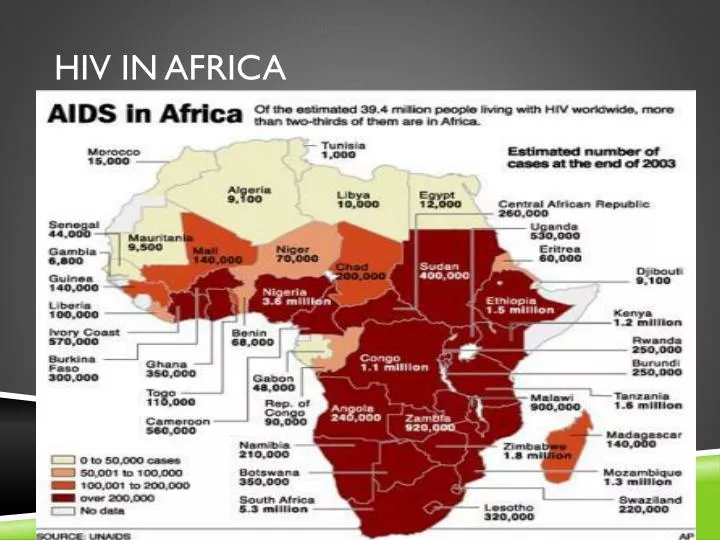
HIV DEATHS • Two-thirds of all people infected with HIV live in sub-Saharan Africa, although this region contains little more than 10% of the world’s population. • During 2009 alone, an estimated 1.3 million adults and children died as a result of AIDS in sub-Saharan Africa. Since the beginning of the epidemic more than 15 million Africans have died from AIDS. • In many countries of sub-Saharan Africa, AIDS is erasing decades of progress in extending life expectancy. In the worst affected countries, average life expectancy has fallen by twenty years because of the epidemic. Life expectancy at birth in Swaziland is just 31 years - less than half of what it would be without AIDS
HIV AND HEALTH CARE • In all heavily affected countries the AIDS epidemic is adding additional pressure on the health sector. As the epidemic matures, the demand for care for those living with HIV rises, as does the toll of AIDS on health workers. • Botswana, for example, lost 17% of its healthcare workforce due to AIDS between 1999 and 2005. • As the HIV prevalence of a country rises, the strain placed on its hospitals is likely to increase. In sub-Saharan Africa, people with HIV-related diseases occupy more than half of all hospital beds
HIV AND FAMILIES • In many cases, the presence of AIDS causes the household to dissolve, as parents die and children are sent to relatives for care and upbringing. • Households in which an adult had died from AIDS were four times more likely to dissolve than those in which no deaths had occurred.
HIV AND FOOD • The AIDS epidemic adds to food insecurity in many areas, as agricultural work is neglected or abandoned due to household illness. • It was calculated in 2006 that by 2020, Malawi’s agricultural workforce will be 14% smaller than it would have been without HIV and AIDS. In other countries, such as Mozambique, Botswana, Namibia and Zimbabwe, the reduction is likely to be over 20%
HIV AND COMMUNITY • Many communities have developed a stigma against HIV patients and are not receiving the proper treatment because of this. • The WHO cites fear of stigma and discrimination as the main reason why people are reluctant to be tested, to disclose HIV status or to take antiretroviral drugs
HIV AND EDUCATION • As the epidemic worsens, the education sector is damaged, which in turn is likely to increase the incidence of HIV transmission. • A decline in school enrolment is one of the most visible effects of the epidemic. • Children may be removed from school to care for parents or family members, or they may themselves be living with HIV. Many are unable to afford school fees and other such expenses – this is particularly a problem among children who have lost their parents to AIDS, who often struggle to generate income.
HIV AND WORK • HIV and AIDS dramatically affect labor, setting back economic and social progress. The vast majority of people living with HIV in Africa are between the ages of 15 and 49 - in the prime of their working lives. • In areas that have been hit hardest by the epidemic, it found that up to 40% of companies reported that HIV and AIDS were having a negative effect on profits. • It is thought that the impact of AIDS on the gross domestic product (GDP) of the worst affected countries is a loss of around 1.5% per year; this means that after 25 years the economy would be 31% smaller than it would otherwise have been.
Campaign to cure • Uganda: Uganda’s first AIDS control program was set up in 1987 to educate the public about how to avoid becoming infected with HIV. • ABC program • Abstinence • Be Faithful • Condoms
Why did it work • Strong political leadership and commitment to tackling AIDS • Free antiretroviral drugs have been available in Uganda since 2004. • President Museveni encouraged input from numerous government ministries, NGOs and faith-based organizations. He relaxed controls on the media and a diversity of prevention messages spread through Uganda's churches, schools and villages. • Music and educational tours by popular musician Philly Lutaaya (who was the first prominent Ugandan to openly declare he was HIV positive) • Many organizations were often made up of people living with HIV educating their peers. These groups worked to break down the stigma associated with AIDS, and encourage an open discussion of sexual subjects that had previously been taboo.
Why is progress stopping • It is thought that the introduction of HIV drugs may have led to complacency about HIV as AIDS is no longer an immediate death sentence. • Significant investment of money for abstinence-only programs from PEPFAR, the American government’s initiative to combat the global HIV/AIDS epidemic has forced the Ugandans to change their program • Uganda’s shift in prevention policy away from ABC may also be responsible for an increase in risky behavior, as comprehensive sex education and condom promotion are no longer mainstream. • The momentum of condom distribution was lost in 2004 when the Ugandan government issued a nationwide recall of the condoms distributed free in health clinics, due to concerns about their quality. • Millions of condoms were incinerated, and by mid-2005 there was said to be a severe scarcity of condoms in Uganda, made worse by new taxes which made the remaining stocks too expensive for many people to afford
Current Uganda • In June 2006, the Ministry of Health announced it had, with assistance from the World Bank, imported 80 million re-branded condoms for free distribution. • However, in 2010 another shortage of free condoms was reported which a Ministry of Health official blamed on the long procurement process, erratic delivery and lack of storage space for condoms • Conflicting messages and problems with distribution appears to have had an effect on the number of people using condoms. UNAIDS found that condom use during sex with non-regular partners was reported by 20 percent, 39 percent, 47 percent and 35 percent of women in 1995, 2000, 2004–2005 and 2006 • http://www.cbsnews.com/video/watch/?id=6362538n&tag=contentMain;contentBody
Links to films • http://www.irinnews.org/film/?id=4210 • http://www.irinnews.org/film/?id=4304 • http://www.irinnews.org/film/?id=4094