Download
1 / 27
310 likes | 858 Views
Neisseria. By: Maria Rosario L. Lacandula,MD,MPH Department of Microbiology and Parasitology College Of Medicine Our Lady of Fatima University. Neisseria. German Physician- A.L.S. Neisser 2 specie- N. gonorrhea N. meningitidis Strict human pathogen Fastidious organism

E N D
Neisseria By: Maria Rosario L. Lacandula,MD,MPH Department of Microbiology and Parasitology College Of Medicine Our Lady of Fatima University
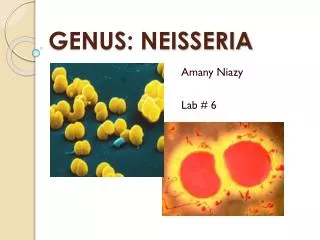
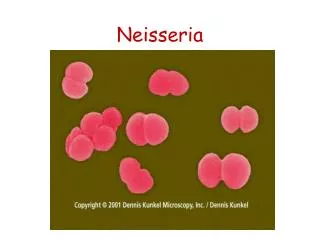
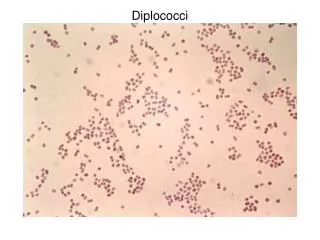
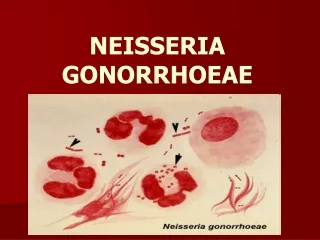
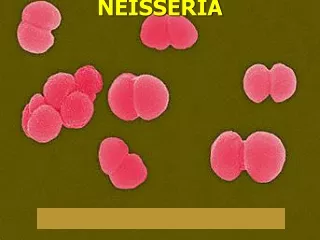
Neisseria • German Physician- A.L.S. Neisser • 2 specie- N. gonorrhea N. meningitidis • Strict human pathogen • Fastidious organism • Aerobic,gram negative cocci, pairs, coffee bean shaped • Non motile, non sporing
Neisseria • Oxidase positive • Acid production by oxidation N. meningitidis- maltose, glucose N. gonnorhea- glucose • Growth-non specific- blood agar specific- Thayer Martin media VCN antibiotics • enhance-exposure to 5% CO2
Neisseria gonorrhea • Optimum growth-tempt. is 35 C to 37 C with poor survival –cool temperature • Structure is typical of Gram negative • Outer surface is not covered with a true CHON capsule
Neisseria gonorrhea • Virulence factors • PILI- fresh clinical isolates • Control by Pil gene • Expression of pili is associated with virulence T1 T2 T3 T4 T5 • Antigenic variation of pili proteins and phase variation of pilin expression
Neisseria gonorrhea • 2.Por proteins • Form pores or channels in the outer membrane • inhibits phagosome lysosomal fusion • Por A- express resistant to serum killing-disseminated disease • Por B • Antigenic variation –serotype classification
Neisseria gonorrhea 3.OPA-opacity protein • Mediates binding to epithelial cells • Opaque colonies • Adherence of bacteria to each other and to eukaryotic cell
Neisseria gonorrhea 4 RMP- reduction modifiable proteins -Stimulate antibodies that block serum bactericidal activity 5. Transferrin binding protein Lactoferrin binding protein Hemoglobin binding protein 6. LOS-endotoxin activity 7. IgA proteases- degrades secretory IgA 8. Beta lactamase- hydrolyzes Beta lactam ring
Neisseria gonorrhea • Epidemiology Transmitted by sexual contact Women 50% risk developing disease after single exposure Men 20% risk developing disease after single exposure The risk of infection increases with more sexual partners
Neisseria gonorrhea Major resorvoir-asymptomatic infected person Asymptomatic carriage-common in women Half of infected women- have mild asymptomatic infection Men-symptomatic Asymptomatic infection- rectal and pharyngeal
Neisseria gonorrhea Clinical Diseases Men-urethritis-urethral d/c and dysuria Complication is rare- epididymitis,prostatitis & periurethral abscesses Women- Cervicitis- infect endocervical columnar epithelial cells. -d/c,dysuria, and abdominal pain 10-20%- ascending infection can occur
Neisseria gonorrhea • 1-3% of infected women-Disseminated infection, infection of skin and joints • Clinical Manifestation of disseminated disease include fever, migratory arthralgias,suppurative arthritis in wrist,knees, ankles and a pustular rash on an erythematous base over the extremities
Neisseria gonorrhea • Other diseases: • Fitz-hugh-Curtis Syndrome • Opthalmia neonatorum • Anorectal gonorrhea • Pharyngitis • conjuctivitis
Neisseria gonorrhea • Laboratory Diagnosis 1.Gram stain- 90% sensitive and 98% specific- symptomatic cases 60% or less- asymptomatic cases -confirmed by culture useful in purulent arthritis 2.Genetic probes- sensitive, specific and rapid 3.Serology- not recommended
Neisseria gonorrhea • Treatment, Prevention & Control Ceftriaxone, cefexime, ciprofloxacin or ofloxacine doxycline or azithromycin 1% tetracycline, 0.5% erythromycin eye oitment
Neisseria Meningitidis • Gram negative diplococci, coffee bean shaped • Encapsulated • Common colonizer of nasopharynx of healthy people • Blood agar- transparent,non pigmented colonies • With large capsule- mucoid
Neisseria Meningitidis • 13 serogroups- antigenic differences on their capsule serogroups- A,B,C,X,Y and W135 • Serotype classification- differences in the outer membrane proteins and oligosaccharide component of LOS • Epidemiologic classification
Neisseria Meningitidis • 4 factors that determine outcome of infection • bacteria colonize the nasopharynx • Specific group and serotype-specific antibodies are present • Systemic spreads occurs w/o Ab mediated phagocytosis • Toxic effects are expressed
Neisseria Meningitidis • Incidence of disease- greatest in children younger than 2 y/o • Def in C5,C6,C7 or C8- increase risk • Toxic effects- LOS endotoxin • Epidemiology -occurs worldwide -epidemics-common in developing countries
Neisseria Meningitidis • Develop countries-serogroup B,C, or Y • Underdevelop countries- serogroup A • Meningococcal pneumonia-serogroup Y and W135 • MOT: respiratory droplets • Humans- natural carriers • School aged children and young adults with high incidence in low socioeconomic group • Common during dry cold months of the year
Neisseria Meningitidis • Clinical Disease • Meningitis -start abruptly with HA,meningeal signs, and fever -neurologic sequelae is low-hearing defects and arthritis • Meningococcemia - septicemia with or w/o meningitis -thrombosis of small bld vessel and multiorgan involvement • DIC with bilateral hge of the adrenals- Waterhouse-Friderichsen syndrome
Neisseria Meningitidis • Pneumonia • Arthritis • Urethritis • Laboratory Diagnosis • Specimens-blood and CSF • Gram stain • Latex agglutination
Neisseria Meningitidis • Treatment -Penicillin - rifampicin or Minocycline- prophylaxis - Vaccine- polyvalent vaccine A,C,Y,W135