Download
1 / 51
2.11k likes | 6.07k Views
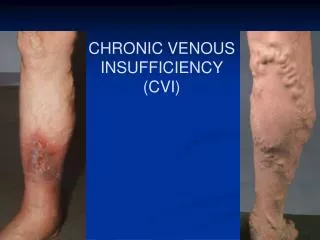
CHRONIC VENOUS INSUFFICIENCY (CVI). CVI. Occurs when the vein valves become dysfunctional and impairs venous blood return. Affects up to 20% of adults. By age 50 ~40% of women and 20% of men have significant vein problems.

E N D
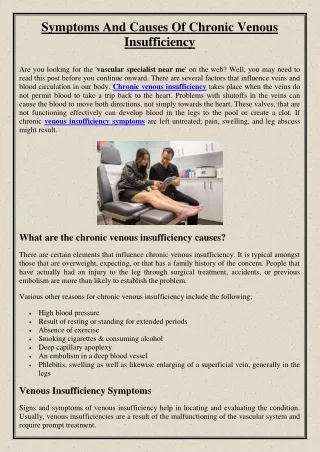
CVI • Occurs when the vein valves become dysfunctional and impairs venous blood return. • Affects up to 20% of adults. • By age 50 ~40% of women and 20% of men have significant vein problems. • More people lose work time from vein disorders then from artery disease. 1.
RISK FACTORS • Advancing age • Family history of venous disease • Ligamentous laxity (eg, hernia, flat fleet) • Prolonged standing • Increased body mass index • Smoking • Sedentary lifestyle • Lower extremity trauma • Prior venous thrombosis (superficial or deep) • Arteriovenous shunt • Hereditary conditions • High estrogen states • Pregnancy 2.
PROGRESSION OF VEIN DISEASE • ASYMPTOMATIC • SUPERFICIAL VENOUS DILATATION Telangiectasias (intradermal) Reticular veins (subdermal)
PROGRESSION OF VEIN DISEASE • ASYMPTOMATIC VS SYMPTOMATIC • VARICOSE VEINS (subcutaneous)
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Leg edema
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Skin changes Hyperpigmentation
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Skin changes Stasis dermatitis
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Skin changes Corona phlebectatica a. venous cups (veins) b. telangiectasias c. reticular veins d. stasis spots (capillaries)
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Lipodermatosclerosis a form of panniculitis just above the ankles. 9.
PROGRESSION OF VEIN DISEASE • CHRONIC VENOUS INSUFFICIENCY • Venous stasis ulceration(s)
EVALUATION • CONSIDER A BIOPSY TO EVALUATE FOR POSSIBLE MALIGNANCY VS INFECTIOUS OR INFLAMMATORY PROCESS. • DOPPLER ULTRASOUND - VENOUS. CONSIDER ARTERIAL DOPPLER IF THERE IS ANY CONCERN OF SIGNIFICANT ARTERIAL OCCLUSIVE DISEASE.
EVALUATION • VENOUS DOPPLER ULTRASOUND Evaluate for deep and superficial venous thrombosis. Evaluate for incompetent veins with significant reflux disease. Evaluate for incompetent perforating veins and tributaries.
VIDEO SHOWING SIGNIFICANT REFLUX DISEASE OF THE GREAT SAPHENOUS VEIN
CLASSIFICATION VEIN DISEASE • CEAP – an international consensus conference initiated the Clinical-Etiology-Anatomy-Pathophysiology classification. • C 0 – no evidence of venous disease. • C 1 – telangiectasias/reticular veins. • C 2 – varicose veins. • C 3 – edema associated with vein disease. • C 4a – pigmentation or eczema. • C 4b – lipodermatosclerosis. • C 5 – healed venous ulcer. • C 6 – active venous ulcer. • E c – congenital • E p – primary venous disease. • E s – secondary venous disorder. • E n – not specified. • A s – superficial veins. • A d – deep veins. • A p – perforating veins. • A n – not specified. • P r – venous reflux. • P o – venous obstruction. • P n – not specified. 7.
MANAGEMENT OF CVI • LEG ELEVATION – heart level for 30 minutes 3-4 times daily improves micro-circulation reduces edema, and promotes healing of venous ulcers.4. • EXERCISE – daily walking and simple ankle flexion exercises.
MANAGEMENT OF CVI • Compression therapy - avoid contraindications such as cellulitis or significant arterial occlusive disease.
MANAGEMENT OF CVI – COMPRESSION THERAPY • Compression bandages – elastic or non-elastic with single or multi-layers.
MANAGEMENT OF CVI • PNEUMATIC COMPRESSION THERAPY
MANAGEMENT OF CVI - MEDICATIONS • Diuretics – one of the most inappropriate treatments. • Aspirin – may accelerate the healing of chronic ulcers. • Pentoxifylline – more effective for complete or partial ulcer healing then placebo. • Stanozolol – an anabolic steroid that stimulates fibrinolysis and improves lipodermatosclerosis and possibly ulcer healing. • Escin (horseshoe chestnut) – 50mg twice daily reduces leg volume and edema. It stimulates the release of F series prostaglandins which induce venoconstriction, decreasing the permeability of vessel walls to low molecular proteins, water, and electrolytes. • Hydroxyethylrutoside, Sulodexide, Prostacyclin Analogues – not available in the United States. 4.
MANAGEMENT OF CVI – SKIN CARE • Skin cleansing – wash with a mild non-soap cleanser (e.g. Dove, Olay, Caress). • Emollients – provides a film of oil to lubricate the skin (e.g. Vaseline, Lubriderm, Aveeno). • Barrier preparations – physically block chemical irritants and moisture.(e.g. Zinc oxide, Vaseline). • Topical corticosteroids – often used to treat stasis dermatitis.4.
MANAGEMENT OF CVI – VENOUS STASIS ULCERS • Surgical debridement – used to remove devitalized tissue. • Enzymatic agents – used to break down necrotic tissue (e.g. Santyl). • Growth factors – synthesized by many cell types such as platelets, neutrophils, and epithelial cells (e.g. Regranex). • Bioengineered tissue – used for a variety of non-healing ulcers (e.g. Apligraf, Dermagraft). • Skin grafting – an option for non-healing ulcers. 4.
MANAGEMENT OF CVI – VENOUS STASIS ULCERS • Dressings – depend upon the ulcer characteristics, frequency of dressing changes, and cost. -Occlusive dressings may be fully occlusive (impermeable to gases and liquids) or semi-impermeable (impermeable to liquids and partially permeable to gases and water vapor). It stimulates collagen synthesis, angiogenesis, and speeds reepithelialization. -Low adherent gauze dressings – frequent changes but inexpensive. -Hydrogels and alginate dressings are highly absorbent to handle heavily exudative ulcers, while hydrocolloids can help with wound debridement and skin protection. -Silver can be incorporated if the ulcer is infected. 4.
MANAGEMENT OF CVI – ABLATION THERAPY • Indications – patients with persistent signs/symptoms of venous disease after a minimum of 3 months of medical therapy (e.g. compression) and documented reflux (e.g. >0.5 seconds of reflux GSV). • Absolute contraindications – acute DVT or phlebitis and pregnancy. 5,6. • Radiofrequency versus laser endovenous ablation therapy.
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY • Radiofrequency devices – generate a high frequency alternating current for which the energy heats the adjacent vein walls to the probe which alters the protein structure of the vein effecting its closure. 5. • Superficial veins include – Great Saphenous Vein, Small Saphenous, and incompetent perforator veins.
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY
MANAGEMENT OF CVI – RADIOFREQUENCY ENDOVENOUS ABLATION THERAPY BEFORE AFTER
MANAGEMENT OF CVI – ENDOVENOUS LASER ABLATION THERAPY • Lasers emit a single, coherent wavelength of light. Laser therapy of venous structures is based upon the concept of selective photothermolysis (ie, selective thermal confinement of light induced damage). Vein wall injury is mediated directly by absorption of photon energy by the vein wall and indirectly by thermal convection from steam bubbles, and from heated blood. • Superficial veins include – Great Saphenous Vein, Small Saphenous Vein, incompetent perforator veins, telangiectasias and reticular veins. 6.
MANAGEMENT OF CVI – MECHANICAL ABLATION • Physical destruction of a vein with its partial or complete removal. - Vein ligation/stripping - Stab phlebectomy - Powered phlebectomy - Open or endoscopic perforator ligation.
MANAGEMENT OF CVI - SCLEROTHERAPY • Chemical irritants injected to close unwanted veins. Preparations include liquid and foam. It is used primarily in the treatment of telangiectasias, reticular veins, and small varicose veins. • These substances cause endothelial damage by their actions as either osmotic or detergent agents. Osmotic agents achieve their effect by dehydrating endothelial cells through osmosis. Detergents are surface active agents which damage the endothelium by interfering with cell membrane lipids. 8.
MANAGEMENT OF CVI - SCLEROTHERAPY • DETERGENT AGENTS - Sodium tetradecyl sulfate - Polidocanol • OSMOTIC AGENTS - Hypertonic saline - Glycerin
REFERENCES • 2012 Vascular Disease Foundation. 8206 Leesburg Pike, suite 301, Vienna Virginia 22187. • Alguire PC, Scovell S. Overview and medical management of lower extremity chronic venous disease. 2012 UpToDate. • Venous stasis and arterial ulcer comparison. February 1, 2009. http://www.lhsc.on.ca/Health_Professionals/Wound_Care/venous.htm. • Alguire PC, Mathes BM. Medical management of lower extremity chronic venous disease. 2012 UpToDate. • Scovell S. Radiofrequency ablation for the treatment of lower extremity chronic venous disease. 2012 UpToDate. • Ihnat DM. Endovenous laser ablation for the treatment of lower extremity chronic venous disease. 2012 UpToDate. • Collins KA. Classification of lower extremity chronic venous disorders. 2012 UpToDate. • Greenberg DL, Scovell S. Liquid and foam sclerotherapy techniques for the treatment of lower extremity veins. 2012 UpToDate. • Alguire PC, Mathes BM. Pathophysiology of chronic venous disease. 2012 UpToDate.