Download
1 / 53
530 likes | 761 Views
EHR Coding Queue. Presenter Elvira Mosely Phoenix Area Office Clinical Program Consultant. Turning on the Coding Que. When does my site need to turn coding que on? As soon as you turn on paperless refill you need to turn on the coding que

E N D
EHR Coding Queue Presenter Elvira Mosely Phoenix Area Office Clinical Program Consultant
Turning on the Coding Que • When does my site need to turn coding que on? • As soon as you turn on paperless refill you need to turn on the coding que • What date should my site use when turning on the coding que? • Use the same date that you use when you turn on paperless refill. • Where does my site turn on the coding que? • See HIM/BO setup power point • Who is responsible for turning on the coding que? • Site manager, CAC, Data Entry Supervisor • Must communicate with Pharmacy or CAC in order to determine when they will implement paperless refill or documenting in EHR
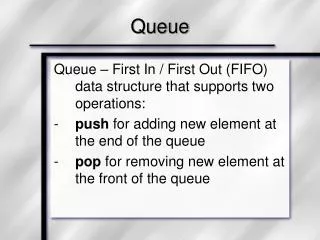
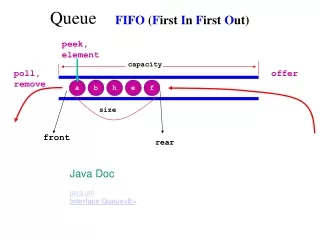
Coding Queue • Captures ALL electronically created visits into a holding que • Prevents visits not reviewed by data entry from passing directly to the billing package • Visits captured include: • Paperless Refills • ALL EHR created visits
How do I get to the Coding Que Menu? • PCC • PCC Management Reports (PCC) • Enter/Modify/Append PCC Data (ENT) • EHR/PCC Coding Audit Menu (EHRC)
(EHRD)Visit by Date Range • Used to audit visits that are created by EHR users • Visit display in list are those with an INCOMPLETE or blank chart audit status • List can be sorted by date, primary provider, clinic code, hospital location (scheduling clinic), & facility
Once the visit is reviewed, the reviewed status can be set to: • Reviewed/Complete • Incomplete • All visits set as reviewed/complete will be passed to the IHS/RPMS billing package • A visit will NOT pass to billing until it is marked reviewed/completed
Incomplete/Orphan ancillary visits: • Will NOT appear on the EHRD report list • These visits will show up on the LIR and the PPPV reports • This type of visits will need to be completed and flagged as complete through the normal data entry process
The EHRD option is where most of your work resides. At this point the coding queue will bring all visit into the queue for coders to review
After selecting my search dates, I would follow the prompts and edit these prompt as appropriate
The system will give you a summary of your choices. You may chose to continue or you may edit your sort fields
When you select display, the system will display your visit similar to the way DVB menu display’s it in PCC
The system will display the note. Coders can view notes in the coding queue or in EHR.
Select Action: D// MOD Modify Visit • Modify which Visit: (1-98): 92 • Looking for ancillary data to merge into this visit... • MNEMONIC: PV Purpose of Visit ALLOWED VISIT RELATED ONLY • 1 .9999 ABBEY,TRESSIA LYNN JAN 26, 2007@09:57 • 2 401.9 ABBEY,TRESSIA LYNN JAN 26, 2007@09:57 • Choose: 1 • POV: .9999// HTN • 401.9 (HYPERTENSION NOS) • UNSPECIFIED ESSENTIAL HYPERTENSION
If I am not ready to release this visit, then I would mark it Incomplete • MNEMONIC: • Looking for ancillary data to merge into this visit... • Do you want to update the Chart Audit Status for this visit? Y// ES • CHART AUDIT STATUS: ? • Choose from: • R REVIEWED/COMPLETE • I INCOMPLETE • CHART AUDIT STATUS: I INCOMPLETE • CHART DEFICIENCY REASON: ?? • Choose from: • ABNORMAL LABORATORY • BLOOD TRANSFUSION • CAUSE OF INJURY • CHIEF COMPLAINT • CONSENT FORM • CONSULTATION REPORT • CPT CODES
When you mark visit incomplete, you need to enter the reason why the visit was not complete. The reason found under this section are editable. • CHART DEFICIENCY REASON: OTHER • Do you want to update the Chart Audit Notes for this visit? N// YES
Adding chart audit notes is a way to communicate important info to other coders • CHART AUDIT NOTES: • No existing text • Edit? NO// Y
Select Action: D// C • 1 Chart Audit History • 2 Change Date/Time • CHOOSE 1-2: 1 Chart Audit History • Display Chart Audit History for which Visit: (1-98): 92 • Chart Audit History for VISIT: • Visit Date: JAN 26, 2007@09:57 Patient Name: ABBEY,TRESSIA LYNN • Hospital Location: FAMILY MED Primary Provider: USER,BSTUDENT • DATE OF AUDIT STATUS USER WHO AUDITED CHART DEFICIENCY • MAR 19, 2007@10:37 INCOMPLETE USER,BSTUDENT OTHER • NOTES: • Waiting for provider to add his note changes before completing the visit • Press Enter to Continue:
Adding chart deficiency reasons • ACDR Add new Chart Deficiency Reason to Table [APCDCAF ADD CHART DEF REASONS] **> Locked with APCDZ ADD CDR
Enter "VA to jump to VIEW ALERTS option Select EHR/PCC Coding Audit Menu Option: ACDR Add new Chart Deficiency Reason t o Table Select OUTPATIENT CHART DEFICIENCY REASONS: ? Answer with OUTPATIENT CHART DEFICIENCY REASONS Do you want the entire 48-Entry OUTPATIENT CHART DEFICIENCY REASONS List? Y (Yes) Choose from: ABNORMAL LABORATORY BLOOD TRANSFUSION CAUSE OF INJURY CHIEF COMPLAINT CONSENT FORM CONSULTATION REPORT History & Physical Initials for Immunizations GIV Initials for Pelvic Exam IV Flow Sheets Lab POV Nursing Assessment Other Pathology Report Pediatric Record Problem List Updates Progress Notes Purpose of Visit Sign OP Report Sign PCC Form – Nursing Sign PCC Form – Pharmacy Sign PCC Form – Primary Provider Time of Visit Transaction Code Unacceptable Abbreviations Vital Signs
(TUR)Count Unreviewed Visits • Reports a count of all visits with a chart audit status of incomplete or blank • Visits can be selected and sorted by: • Date • Primary provider • Chart audit status. • Contract Health Visits are EXCLUDED
Mar 19, 2007 Page: 1 • PCC Data Entry Module • ****************************************************************** • * COUNT OF VISITS WITH CHART AUDIT STATUS OF INCOMPLETE/BLANK * • ****************************************************************** • VISIT Date Range: NOV 19, 2006 through MAR 19, 2007 • VISIT DATE SERV CAT # UNREVIEWED VISITS # W/NO PROV • (ANCILLARY) • ------------------------------------------------------------------------------- • Nov 21, 2006 AMBULATORY 1 • Nov 27, 2006 AMBULATORY 2 • Nov 28, 2006 AMBULATORY 2 • Nov 29, 2006 AMBULATORY 1 • Dec 04, 2006 AMBULATORY 1 • Dec 06, 2006 AMBULATORY 1 • Dec 07, 2006 AMBULATORY 2 1 • Dec 12, 2006 AMBULATORY 2 • TELECOMMUNIC 1 • Dec 19, 2006 AMBULATORY 1 1
CASP Update EHR Coding Audit Site Parameters • EHR Coding Queue Parameter Update • Select PCC DATA ENTRY SITE PARAMETERS SITE NAME: DEMO HOSPITAL// NASHVILL • E NON-IHS CHEROKEE 01 NM HOSPITAL 1601 • Service Category exclusions: If you would like to exclude • visits with a particular service category from the list of • visits displayed in the coding queue you must enter those • service categories to the list below. For example, if you • do not wish to have I - In Hospital visits in the list then • you should add 'I' to the list. • Please note: If you leave the list blank (empty) then all • direct (non-CHS) visits will display in the coding queue. • Event visits never display in the coding queue. • Your site is currently set up to exclude visits with the • following service categories from the coding queue: • I - IN HOSPITAL • H - HOSPITALIZATION • D - DAILY HOSPITALIZATION DATA • O - OBSERVATION • R - NURSING HOME • Select one of the following: • A Add another service category to the list • R Remove a service category from the list • Q Quit - list looks good • Do you wish to: Q//
Continues • Do you wish to: Q// uit - list looks good • You have the option of seeing all visits in the coding queue • regardless of how they were created. You can see all visits or • limit the list of visits in the coding queue to only those • on which a provider has been entered. If you choose to only • see visits on which a provider was entered then you will not • see visits that were created by an ancillary package. Most, • if not all visits created by EHR users will have provider. • Include all visits in the coding queue list?: YES, INCLUDE VISITS WITH NO PROVID • ER//
You can change the default to no • Default Response for 'Is Coding Complete?' in Data Entry: ? • Choose from: • Y YES • N NO
Recommendations • All visits should be completed REGARDLESS if they are billable or not • When documenting chart deficiency reasons try not to select OTHER • Not enough information for other coders or supervisors reviewing incomplete visits in the future.