Download
1 / 18
190 likes | 672 Views
Leukemia. Maturation of Myeloid Cells. Dr. Rania Alhady. Leukemia. * Definition of leukemia: Leukemia is malignant proliferation of hematopoietic cells in the bone marrow followed by blood dissemination and soft tissue infiltration. • Leukemic cells produce symptoms because of:

E N D
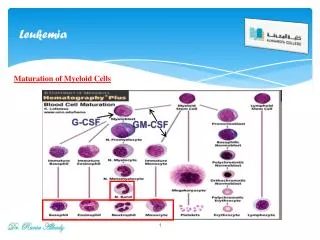
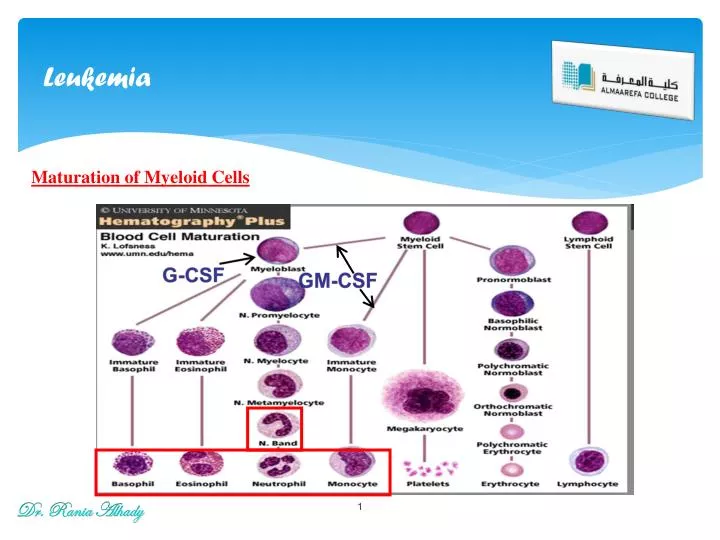
Leukemia Maturation of Myeloid Cells Dr. Rania Alhady
Leukemia * Definition of leukemia: Leukemia is malignant proliferation of hematopoietic cells in the bone marrow followed by blood dissemination and soft tissue infiltration. • Leukemic cells produce symptoms because of: (i) Bone marrow failure (i.e. anemia, neutropenia, thrombocytopenia) and (ii) Infiltration of body organs (e.g. liver, spleen, lymph nodes, meninges, brain, skin or testes). * Classification of leukemia: 1. Acute Leukemia: • Acute lymphoblastic leukemia (ALL): L1 – L3. • Acute myeloblastic leukemia: (AML): M0 – M7. 2. Chronic Leukemia: • Chronic lymphocytic leukemia (CLL). • Chronic myelocytic leukemia (CML). Dr. Rania Alhady
Leukemia * Etiology of leukemia: 1. Congenitaldisorder: Down syndrome, Immunodeficiencysyndrome. 2. Ionizing radiation: X-ray, radiotherapy. 3. Chemicals: (alkylating agent, Benzene). 4. Viruses: HumanT-lymphocyte leukemia virus (HTLV1), Herpes virus, EBV.
Acute leukemia Acute Leukemia - Uncontrolled proliferation of leukemic (blast cells) in bone marrow, and followed by infiltration of peripheral blood and soft tissues (lymph nodes, spleen, liver, meninges, gum……). N.B: • Blast cells in bone marrow must be > 30% to diagnose acute leukemia. • Acute leukemiasare fatal if not treated. • However, acute leukemias are easier to treat than chronic leukemias. Dr. Rania Alhady
Acute leukemia * Classification of acute leukemia: - Acute leukemias are classified according to the type of blast cells into: 1. Acute lymphoblastic leukemia (ALL): Childhood leukemia. 2. Acute myeloblastic leukemia (AML): Adulthood leukemia. Dr. Rania Alhady
Acute Lymphoblastic Leukemia Acute Lymphoblastic Leukemia (ALL): • It is the result of clonal proliferation of lymphoid progenitor cells (B or T lymphoblast) originating in the bone marrow. • About 85% of ALL are of B type, occurs in children, characterized by extensive bone marrow infiltration and variable peripheral blood involvement. • About 15% of ALL are of T type, occurs in adolescents characterized by extensive thymic gland infiltration and marked peripheral blood involvement. • Malignant B and T lymphoblasts are also morphologically indistinguishable, and subclassification of ALL is thus dependent on immunophenotyping according to the French-American-British (FAB) classification system into L1, L2 and L3. Dr. Rania Alhady
Acute Lymphoblastic Leukemia * Clinical features of ALL: 1- Bone marrow failure: • RBCs → Anemia: pallor, lethargy, malaise and dyspnea. • Leukocytes → neutropenia: fever, malaise, features of mouth, skin, respiratory infections. • Platelets → throbombocytopenia: spontaneous bruises, pupura, bleeding gums. 2- Tissue infiltration: • L.N. enlargement. • Hepatomegaly. More common with ALL than AML. • Splenomegaly. 3- Organ infiltration: A- Bony infiltration. B- Testicular infiltration. C- C.N.S. infiltration. 4- Fever. Dr. Rania Alhady
Acute Lymphoblastic Leukemia * Investigations of ALL: 1. CBC: • 60% of patients have an elevated ↑↑ WBCs. • RBCs: ↓ Hb • Platelets: ↓ • Neutrpenia • 90% have lymphoblastsin the peripheral blood film. 2. Bone marrow: BM Aspirate: • Hypercellular BM • All normal marrow elements are depressed and replaced by abnormal blasts. • 30% or more of all nucleated cells are blast Dr. Rania Alhady
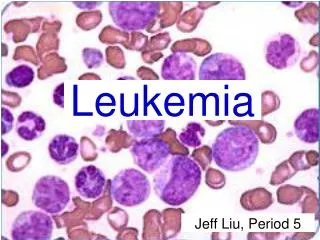
ALL: Lymphoblastshave condensed chromatin, inconspicuous nucleoli, and scant agranular cytoplasm
Acute Lymphoblastic Leukemia (a) L1 subtype-blasts show scanty cytoplasm without granules. (b) L2 subtype-blasts are larger and heterogeneous with more abundant cytoplasm. (c) L3 subtype-blasts are deeply basophilic with cytoplasmic vacuolation. Dr. Rania Alhady Morphological classification of ALL L1 L2 L3
Acute Lymphoblastic Leukemia 3- Immunophenotyping: - Detection of the Antigen present in the cell membrane of the blast cells. A- Myeloid markers:-veCD13, CD33 B- Pan B markers:+veCD19, CD20. C- Pan T markers: +veCD2, CD5, CD7 4- Cytogenetics: • Philadelphia chromosome translocation t (9; 22): may occur and results in poor prognosis. Dr. Rania Alhady
Acute Lymphoblastic Leukemia Prognosis of ALL: Bad prognosis in: WBCs count: ↑ > 20.000 Sex: boys due to testicular involvement. L2 & L3morphology. Organomegaly. Cytogenetic abnormalities (philadelphia chromosome). Pre-T ALL Dr. Rania Alhady
Acute Myeloid Leukemia Acute Myeloid Leukemia (AML) * Definition: - Malignant proliferation of myeloid precursor cells with reduced capacity to differentiate into more mature cellular elements. * Incidence: Acute myelogenousleukemias affect primarily adults, peaking in incidence between the ages of 15 and 39 years, but are also observed in older adults and children. Dr. Rania Alhady
Acute Myeloid Leukemia * Diagnosis: • Clinical Picture: • Anemia weakness and easy fatigue • Neutropenia infections • Thrombocytopenia gingival bleeding, ecchymoses, epistaxis, menorrhagia • Anorexia, weight loss, fever. • Organomegaly: - Hepatosplenomegaly (HSM): in 1/3 of patients. - Lymphadenopathy: is uncommon except in monocytic variants. Dr. Rania Alhady
Acute Myeloid Leukemia B. Laboratory diagnosis: 1. Bone Marrow Exam: • The diagnosis of AML is based on the detection of myeloid blasts which make up more than 20% of the cells in the bone marrow. • Myeloblastshave delicate nuclear chromatin, two to four nucleoli, and more voluminous cytoplasm than lymphoblasts. 2. Immunophenotyping: +ve Pan myeloid markers: CD13, CD33 Dr. Rania Alhady
Acute Myeloid Leukemia * FAB Classification of AML: AML is divided into eight (M0 to M7) categories.This scheme takes into account both the degree of maturation (M0 to M3) and the lineage of the leukemic blasts (M4 to M7). M0: minimally differentiated AML. M1: without maturation AML. M2: with maturation AML. M3: promyelocytic AML. M4: myelomonocytic AML. M5: monocytic AML. M6: erythroleukemia AML. M7: megakaryoblastic AML. Dr. Rania Alhady
Acute Myeloid Leukemia * Prognosis of AML: • AML is a difficult disease to treat. Approximately 60% of the patients achieve complete remission with chemotherapy.