Download
1 / 31
320 likes | 691 Views
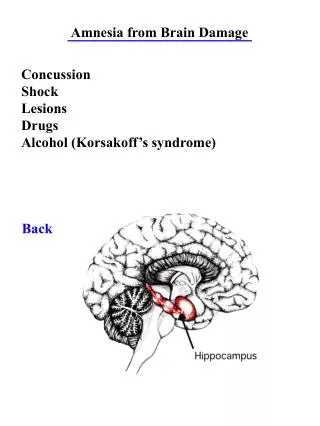
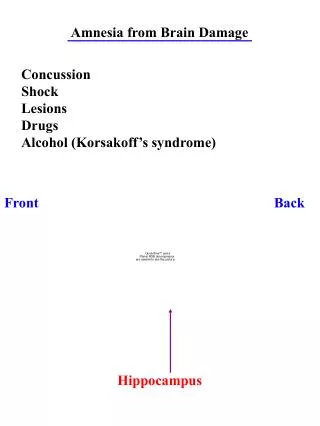
Alcohol Related Brain Damage. ARBD. Wernicke-Korsakoffs: Clinical Characteristics. Acute presentation (Wernicke’s): Ataxia Global confusional state Opthalmaplegia (Abducens and conjugate gaze palsy ; 6 th crainial) Nystagmus Classical triad only occurs in 10% of cases

E N D
Wernicke-Korsakoffs: Clinical Characteristics Acute presentation (Wernicke’s): • Ataxia • Global confusional state • Opthalmaplegia (Abducens and conjugate gaze palsy ; 6th crainial) • Nystagmus Classical triad only occurs in 10% of cases • Also: memory problems, vomiting, lethargy and hypotension, peripheral neuropathy, malnutrition Chronic /residual (Korsakoffs) • Difficulty in learning new information • Preservation of immediate recall • No significant retrograde amnesia • Confabulation (often associated with translocation in time of genuine past experiences, may be grandiose) • Emotional disturbances; apprehension, anxiety, excitability • Hallucinations (sometimes)
Alcohol Related Dementia Cognitive characteristics • Inaccurate memories, confabulation • Disorientation • Verbal and visual processing problems • Inability to screen out irrelevant information • Attention • Planning • Judgement • Processing new information • Apathy • Poor motivation • Neglect • Disinhibited • Impulsive
ARBD Brain Injury/infarction ARD WE Neuro syndromes
Prevalence2ndry care studies • Harvey 1998 (hospital records <65s) (prospective study of all identified cases in 2 London areas over two years) • EOD: 67.2/100,000 aged 30-64 • 34% Alzheimer's • 18% vascular • 12% front temporal • 12.5% ARBD (peak between 50-60 years old) • Smith and Atkinson 1995 • 21-24% alcohol is a contributing factor in all dementias
Prevalence overview • Prevalence rates are very variable • Condition is under-diagnosed • From a secondary care view point Harvey’s results are probably the most useful • Women more vulnerable than men with earlier onset. • Prevalence likely to reflect socio-economic deprivation and nutritional status • 35 units per week, for five years
Outcomes • Smith and Hillman (1999) • 25% make a complete recovery • 25% make significant recovery • 25% make slight recovery • 25% make no recovery
Qualitative research project • Steering committee • Research commissioned by CSIP (Care Services Improving Partnership) • 13 people with diagnosed alcohol related brain damage, identified through specialist care provision service (Carenza care)
The patients’ perspective • Being passed from pillar to post between services both before and after diagnosis. • Not being given information about Korsakoff’s disease • A perception of Health Professionals that ARBD is self–inflicted and therefore not worthy of an empathic approach • A general view that recovery is not possible with ARBD • The only option for care for someone with ARBD is an Older People’s Mental Health Nursing Care Home
Summary findings • ARBD is stigmatised; • Self inflicted • Low priority • Double jeopardy; dementia and alcohol dependency • Lack of professional responsibility for care • Lack of training in medical professions • Evidence of no clear clinical pathway • Lack of commissioning of care
Pilot service • Nurse and social worker embedded into EOD team • Designed to • Optimise function and quality of life of the patient • Prevent recurrent hospital re-admission • Targeting; • Under age of 65 • Inpatients on acute medical and surgical wards • History of excessive alcohol drinking • Multiple admissions or long stays post medical stabilisation • Evidence of confusion • Post withdrawal • Not currently drinking (whilst in hospital)
Rehab programme • Socialisation • Social contacts • Relationship development • Behavioural • Graded task • Activity scheduling • Cognitive restructuring • Diary keeping • Memory aids • Planning • Problem solving
Categorisation of progress/outcome. • Stabilisation • Period in which the patient is withdrawn from alcohol and physically stable. Cognitive status confirmed and diagnostic formulation established. • Rehabilitation • Psycho-social rehabilitation and cognitive restructuring so as to regain optimum function • Maintenance • Cognitive function stabilised at optimum level and settled in appropriate supportive environment • Discharge • Relapse • Recommenced uncontrolled drinking, periods of acute cognitive disturbance and evidence of progressive cognitive deterioration related to drinking. • Death
Review • 19 cases • Average age: 57 • Gender: 6 female 13 male • Six cases have experienced a major psychotic illness whilst under care: • Alcoholic hallucinosis • Bipolar affective disease • Depression.
Clinical outcomes 19 cases reviewed • 7 cases in rehab • 8 cases in maintenance • 3 cases dead (3 maintained) • 1 case relapsed
Service utilisation Reduction from 31 inpatient days per year prior to engagement with service to 6 inpatient days per year • 6 Team support alone • 2 Direct payments and team support • Enhanced domiciliary care plus team support • Residential supported living • OPA • Partner support • 6 Specialist unit (working age adult unit/alcohol specialist unit)
Capacity and MHA issues Of 30 cases for which we have audit data: • 28 had significant cognitive impairment for at least six months post assessment. • 14 are currently being managed under mental capacity act due to lack of capacity relating to managing their money and aspects of accommodation choices. • Guardianship used in one case, CTO in one case, acute admissions under MHA; 5 cases • Alcoholic hallucinosis • Bipolar affective disorder • Depression.
Main issues • Issues relating to choices about whether the individual understands the implications of continuing to consume alcohol • Alcohol dependency (denial) • Cognitive problems associated with understanding implications (dysexective syndrome and memory problems)
Case study 1 • 51 year old man • Highly intelligent, company director • Married, 3 children • Started drinking 1995 • Multiple hospital admissions (15) excluding periods in private alcohol dependency units. • Pancreatitis, hepatitis, vomiting blood, malnutrition • One period of WE a year ago
Case study 1 Story concerning this admission: • Admitted to medical ward following head injury (fall) • Fronto temporal contusion and fracture with evidence of infarct • GGT >1000 • Physically stabilised: neuro-rehab. • Noted to have cognitive damage prior to discharge home • Managed at home one week; re-admitted, acute alcohol intoxication. • Psychiatry liaison; referred to EOD service. • Guardianship to specialised rehabilitation unit
Case study 1 • Very good progress, cognitive impairments improved, self catering in structured environment • Appeal maintained guardianship
Case study 1Neuropsychological report • IQ 106 • Performance 20points lower than predicted value • Processing speed much reduced: leading to missing information • Perceptual organisation low; ‘difficulty in seeing the whole picture’ • Graded naming was good • Problem solving tests (behavioural assessment of dysexecutive syndrome): proneness to break rules, problems in planning • Sentence completion is very poor due to inability to inhibit responses.
Case study 1 • He has frontal dysexecutive syndrome likely to influence decision making, planning and ability to undertake alcohol rehabilitation • This may be due to brain injury but progressive improvement in abstinence indicates alcohol
Case study 1 • Following 6 months in cognitive rehab centre; • Trial at home with three supportive visits a day • Lasted two weeks • Re-admitted due to drinking • Admission to residential alcohol rehab unit • 4 Months later discharged home on section 25 with 6 has support a day • Lasted two weeks, small amount of drink led to convulsions • Re-admitted, no withdrawal • Discharged with same amount of support, 3 months later still in community • 6 months later ; sudden death…haematemasis
Case study 2 42 year old women Found by police in a skip after sexual assaults No relatives Long standing drinking Multiple hospital admissions including periods in acute hospitals. Protracted malnutrition and chronic liver disease Previous periods of WE a year ago
Neuropsychological profile Profound problems in learning new information Retrograde amnesia Varying confabulation Processing speed much reduced: leading to missing information Perceptual organisation low; ‘difficulty in seeing the whole picture’ Graded naming was good Problem solving tests (behavioural assessment of dysexecutive syndrome): proneness to break rules, problems in planning Sentence completion is very poor due to inability to inhibit responses.
Case study 2 Story concerning this admission: Admitted to medical ward Fronto temporal contusion and fracture with evidence of infarct/brain injury GGT >1000 Physically stabilised Psychiatry liaison; referred to service. Guardianship to specialised rehabilitation unit 3 months Placed in mental health sheltered accommodation under guardianship with rehab package
Case study 2 Very good progress, cognitive impairments improved, self catering in structured environment. Alcohol free Appeal maintained guardianship Maintained in community sheltered accommodation General improvement in independence and memory. Rehabilitative support withdrawn Quality of life good, guardianship closed
Overview • ARBD is an acquired brain injury engendered through excessive alcohol ingestion. Its management has some similarities to that of other acquired brain injury. • Currently there are no national guidelines for the management of ARBD • There is no ‘therapeutic ownership’ or commissioning of ARBD: • Old age services • Alcohol and drug dependency services • Neuropsychiatric services • General adult service • Very few services are commissioned in England • ARBD is not a common problem but patients require significant psycho-social care (high mortality and morbidity). • Therapeutic service are likely to be cost neutral or potentially cost efficient.