Download
1 / 89
1.15k likes | 2.69k Views
Radiology of the Foot. Mark Wahba X-Ray rounds July 24th, 2003. Goals. Approach to radiography of the foot Become familiar with a Lisfranc injury Become familiar with a Jones fracture. Outline. Bones Views Important Points Lisfranc Joint Jones fracture Films. The foot. 28 bones

E N D
Radiology of the Foot Mark Wahba X-Ray rounds July 24th, 2003
Goals • Approach to radiography of the foot • Become familiar with a Lisfranc injury • Become familiar with a Jones fracture
Outline • Bones • Views • Important Points • Lisfranc Joint • Jones fracture • Films
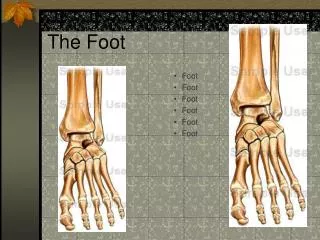
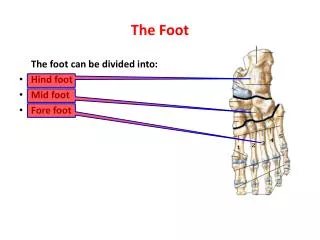
The foot • 28 bones • 57 articulations
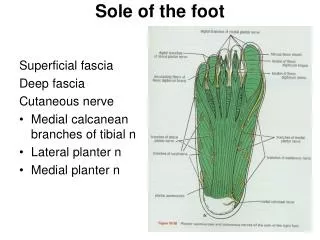
3 anatomic and functional regions • Hindfoot: talus, calcaneus • Midfoot: navicular, cuboid, cuneiforms • Forefoot: metatarsals, phalanges, sesamoids
Accessory Ossification Centres • Normal • 30% of population • Smooth corticated surfaces
Adequate views • Anterior-Posterior • Oblique • Lateral
AP view • Medial margin of the base of the 2nd metatarsal is in line with the medial margin of the middle cuneiform • Base of the 3rd metatarsal is obscured • View 1st and 2nd MT, medial and middle cuneiform
Oblique view • Medial margin of the base of the 3rd metatarsal should be in line with the medial margin of the lateral cuneiform • Base of the 2nd metatarsal is obscured • View 3,4,5 MT, lateral cunieform, navicular, cuboid
Lateral • Hindfoot • Soft tissues • View articulations: CalCub, TN, NCun
Bohler’s Angle • Draw a line from the posterior aspect of the calcaneum to its highest midpoint • Draw a line from the anterior aspect of the calcaneum to its highest midpoint • Measured angle is from 20-40 degrees
Lisfranc Joint • named for Jacques Lisfranc (1790-1847), a field surgeon in Napoleon's army • “described an amputation performed through this joint because of gangrene that developed after an injury incurred when a soldier fell off a horse with his foot caught in the stirrup” • refers to the articulation involving the first and second metatarsals with the medial and middle cuneiforms
Any injury to this area, whether dislocation or fracture-dislocation, is termed a Lisfranc injury • Initially missed 20% of the time • high risk of chronic pain and functional disability if they go unrecognized
Presentation • Hx of Direct trauma • Hx of Indirect trauma: “force is transmitted to the stationary foot so that the weight of the body becomes a deforming force by torque, rotation or compression” • Pain in midfoot • Inability to weight bear, especially on toes • Lisfranc Injury of the Foot: A Commonly Missed Diagnosis, BURROUGHS et al., American Family Physician, July 1998, 58 no. 1 ,p.118
Why? • “While transverse ligaments connect the bases of the lateral four metatarsals, no ligament exists between the first and second metatarsal bases. The joint capsule and dorsal ligaments form the only minimal support about the Lisfranc joint, creating a "weak link" that is prone to injury.” • http://emedhome.com/case-archivedata.cfm?ID=case120701
Almost invariably involve metatarsal fractures • Usually the 2nd metatarsal • # cuboid, cuneiform, navicular occur in 39% • Weight bearing views are useful
Signs of a Lisfranc injury • The medial shaft of the 2nd metatarsal should be aligned with the medial aspect of the middle cuneiform on the AP view. • The medial shaft of the 3rd metatarsal should be aligned with the medial aspect of the lateral cuneiform on the oblique view. • The first metatarsal cuneiform articulation should have no incongruency. • The presence of small avulsed fragments ("fleck sign")should be sought in the medial cuneiform-second metatarsal space. • The naviculocuneiform articulation should be evaluated for subluxation. • Should be no "step-off" as each metatarsal shaft should never be more dorsal than its respective tarsal bone • http://emedhome.com/case-archivedata.cfm?ID=case120701
Jones Fracture • “Sir Robert Jones described his own fracture of the fifth metatarsal in 1902, when he injured himself while dancing around a Maypole at a military garden party” • # at base of 5th metatarsal at metaphyseal-diaphyseal junction
w/in 1.5 cm distal to tuberosity of 5th metatarsal • Should not be confused w/ more common avulsion # of 5th metatarsal tuberosity • An oblique radiograph is essential to accurately assess this fracture
trauma site corresponds to the area between the insertion of the peroneus brevis and tertius tendons • peroneus tertius originates on anterior aspect of fibula • injury occurs when the ankle is plantar flexed and a strong adduction force is applied to the forefoot
Ortho follow up • NWB cast 6-8 weeks • Notorious for nonunion and needing ORIF b/c of low vascularization and high stresses at this site
aka Dancer’s Fracture • Conservative treatment 4-6 wks • Cast, brace, crutches, wooden soled shoe
Thought to occur due to stress on the plantar aponeurosis causing an avulsion • Fractures of the Fifth Metatarsal Yu W. D. et al, THE PHYSICIAN AND SPORTSMEDICINE - VOL 26 - NO. 2 - FEBRUARY 98
Apophysis of 5th metatarsal • “bony outgrowth that has never been entirely separated from the bone of which it forms a part” • Found in the skeletally immature
Stress fracture • a stress phenomenon at the metaphyseal-diaphyseal junction • “severe intramedullary sclerosis, profound thickening of both the medial and lateral cortices, lucency in the lateral cortex”
Treat conservatively or operatively depending on activity level