Download
1 / 30
300 likes | 456 Views
Maine PCMH Pilot Phase 2 Expansion Introduction. Objectives. Welcome! Brief overview Maine PCMH Pilot Review benefits and expectations for Phase 2 practices Preparing to join Pilot – next steps. Why We’re Here. Maine’s Medical Home Movement. ~ 540 Maine Primary Care Practices .

E N D
Maine PCMH Pilot Phase 2 Expansion Introduction
Objectives • Welcome! • Brief overview Maine PCMH Pilot • Review benefits and expectations for Phase 2 practices • Preparing to join Pilot – next steps
Maine’s Medical Home Movement ~ 540 Maine Primary Care Practices 100+ Nat’l Committee for Quality Assurance (NCQA) PCMH Recognized Practices ~130+ MaineCare Health Home-eligible Practices 14 FQHCs CMS Advanced Primary Care (APC) Demo 26 Maine PCMH Pilot Practices 50 Pilot Phase 2 Practices 4
Maine PCMH Pilot Leadership Maine Quality Forum Maine Health Management Coalition Maine Quality Counts MaineCare
Maine PCMH Pilot Key elements: • Convened by Maine Quality Forum, Maine Quality Counts, Maine Health Management Coalition • Originally, 3-year multi-payer PCMH pilot (now 5 yrs) • Collaborative effort of key stakeholders, major payers • Use common mission & vision, guiding principles for Maine PCMH model • Phase 1 includes 22 adult/ 4 pediatric PCP practices across state • Practices receive support for practice transformation & shared learning • Pilot committed to engaging consumers/ patients at all levels • USM Muskie team conducting rigorous outcomes evaluation (clinical, cost, patient experience of care)
Maine PCMH Pilot Practice “Core Expectations” • Demonstrated physician leadership • Team-based approach • Population risk-stratification and management • Practice-integrated care management • Same-day access • Behavioral-physical health integration • Inclusion of patients & families • Connection to community / local community resources • Commitment to waste reduction • Patient-centered HIT
Maine PCMH Pilot – Payment Model 9 • Major private payers participating + Medicaid + Medicare (MAPCP demo) • 3-component PCMH payment: • NEW prospective (pmpm) PCMH care management payments – approx $3pmpm commercial payers & Medicaid; $7pmpm Medicare • Ongoing FFS payments • Ongoing health plan performance payments for meeting quality targets (i.e. existing P4P programs)
But What Does it All Mean - to Patients? • Vision for Change – Phase I Teams (June 09) • “They were here for me” • “Everybody here feels like family” • “They really help us get through the system” • “I feel well cared for in my practice” • “They know what I need and when I need it” • “I don’t feel so alone or anxious anymore” • “Wow – all my needs were met!”
CMS MAPCP Demo • Medicare (CMS) Multi-Payer Advanced Practice (MAPCP) “medical Home” Pilot • Medicare joined Pilot a payer • Allowed introduction of Community Care Teams • Stronger focus on reducing waste & avoidable costs – particularly readmissions • Ability to access Medicare data for reporting, identifying pts at risk • Opportunity for 50 additional practices to join “Phase 2” of Pilot (Jan 2013)
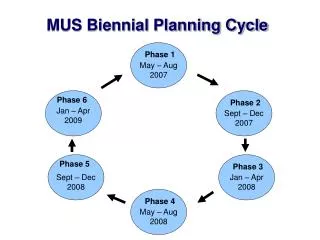
Maine PCMH Pilot - MAPCP Timeline Jan 1, 2010 2011 2012 2013 Dec 31, 2014 ME PCMH Pilot - Original Jan 1, 2012 MAPCP Demo – 3yr ME PCMH Pilot - Extended Dec 31, 2014 Pilot Expansion 12
Multi-Payer Pilot Phase 2 Expansion • 107 practices applied; 84 qualified for multi-payer Pilot • Expectations: • Strong leadership for change • NCQA PCMH recognition (Level 1 or higher)- complete status survey by July 18th • Fully implemented Electronic Medical Record (EMR) • Commitment to implement Pilot Core Expectations • 50 new adult practices selected for participation in multi-payer Pilot, highly competitive process!
Maine PCMH Pilot – Existing + 50 Expansion Practice Sites 14
Community Care Teams 15 • Multi-disciplinary, community-based, practice-integrated care teams • Build on successful models (NC, VT, NJ) • Support patients & practices in Pilot sites, helping patients overcome barriers to care, improve outcomes • Receive pmpm payments from Medicaid, Medicare, commercial payers • Key element of cost-reduction strategy, targeting high-cost patients to reduce avoidable costs (avoidable ED use, admissions)
Maine PCMH Pilot Community Care Teams Schools Transportation Environment • Community Care Team Housing Outpatient Services Workplace Care Mgt Family Food Systems High-need Individual PCMH Practice Med Mgt Specialists • Community Resources Shopping Coaching Hospital Services Behav. Health & Sub Abuse Income Physical Therapy Heat Literacy Faith Community
Eligibility Maine PCMH Pilot Expansion • Practice meets MaineCare Health Home requirements • Adult primary care practice site with at least one full-time primary care physician or nurse practitioner • Practice site does not currently participate in the CMS FQHC Advanced Primary Care (APC) Demonstration • Minimum patient panel of 1000+ patients enrolled in Pilot health plans (Anthem BCBS, Aetna, Harvard Pilgrim Health Care, MaineCare, and Medicare). • Completion of Maine PCMH Pilot Phase 2 Expansion “Memorandum of Agreement” (MOA) • Agreement to contribute modest PMPM toward practice transformation support
What It Means for New Practices • Practices joining multi-payer PCMH Pilot in January 2013 will receive… • New PCMH payments from participating payers • Medicare, Medicaid (HH), Aetna, Anthem, HPHC • Community Care Team support for highest needs pts • Practice transformation support (fee required) • Expectations • Commitment to implement Pilot Core Expectations, demonstrate improvements in quality & cost savings • Contribute practice transformation support fee
Pilot Participation Requirements • Baseline on-site practice assessment • Expectation outlined in original MOA • Intended to identify practice PCMH strengths & opportunities for improvement • Pilot supports 50% costs; practices required to support remaining 50% (est’d ~ $500) • Scheduled as 2 d visit in practice (Sept – Dec) • Aiming for reports back to all practices before Jan 2013
Pilot Participation Requirements • Leadership team to attend Learning Sessions • 3 sessions/year (Feb – June – Oct) – dates TBD! • Will be held in 1 central location (alternate Augusta/Bangor/other?) • At least 3 team members must attend (up to 5 team members may attend) • Participate in monthly leadership webinars • Work collaboratively with QI Coach • Submit bi-monthly Core Expectation Status Rpts • Submit quarterly Clinical Outcomes Data Rpts
Pilot Participation Requirements • Practice Transformation Support fees • CMS requirement to provide same level of practice transformation support as Phase 1 • Supports • Central project management • QI coaching • PCMH Learning Collaborative & Learning Sessions • Webinars, web-based tools • Est’d to be $0.25pmpm ($3pmpy), based on panel sizes reported in practice application
Lessons from 1st PCMH Demo • Becoming a PCMH requires transformation (not incremental change) • Technology needed for PCMH is not “plug & play” • Transformation to PCMH requires personal transformation (esp. physicians!) • Change fatigue is serious concern • Transformation to PCMH is developmental process, & local process • The medical home is not something that can be “installed”
Lessons Learned fromMaine PCMH Pilot • Change starts with effective leadership – clinician, administrative, and organizational • Recognize risks of “change overload” – need to focus, prioritize, sequence change efforts • Recognize that successful change happens only through effective teams (make changes with people, not to people) • Recognize value of external & internal QI coaching
Change is Hard • Hard to change your shorts while running! (and hard to practice while practicing) • PCMH requires practice and personal change • People fear change (loss) - any change
Sustaining Change is Even Harder! • PCMH requires transformation, not incremental change • Making many changes is harder than single change • Sustaining change can be exhausting • Marathon, not a sprint!
Next Steps • Participate in practice on-site assessment (Sept-Dec) • Attend monthly “ramp-up” team calls/webinars (2nd Thurs each month, 7:30A & 4:30P) • Plan for leadership team to attend Expansion Launch – November 16, 2012 Augusta Civic Center • Hold your own team meetings (ideally, weekly!), spread communications about Pilot across team
Summing Up: Medical Home Is Where… • Patients feel welcomed • Staff takes pleasure in working • Physicians feel energized every day 28
Contact Info / Questions 30 • Maine PCMH Pilot: www.mainequalitycounts.org (See “Major Programs” “PCMH Pilot”) • PCMH • Nancy Grenier, RN: ngrenier@mainequalitycounts.org, tel 240.8767 • Kaleigh Sloan, MPH: ksloan@mainequalitycounts.org , tel 622.3374 X 220 • Lisa Letourneau MD, MPH: LLetourneau@mainequalitycounts.org • CCTs: Helena Peterson: hpeterson@mainequalitycounts.org, tel. 266-7211 • MaineCare Health Homes • Michelle Probert: michelle.probert@maine.gov , tel. 287-2641