Download
1 / 31
390 likes | 877 Views
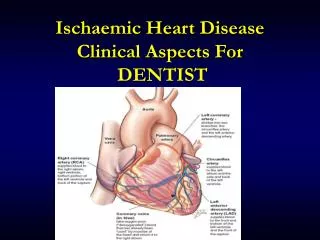
Ischaemic Heart Disease CASE A. CASE A:. Mr HA, aged 60 years, was brought in to A&E complaining of chest pain, nausea and a suspected AMI. The Biochemical Markers. Creatinine Kinase: Biochemical marker of myocardial damage.

E N D
CASE A: • Mr HA, aged 60 years, was brought in to A&E complaining of chest pain, nausea and a suspected AMI.
The Biochemical Markers • Creatinine Kinase: Biochemical marker of myocardial damage. • CK is a ubiquitous enzyme found in nearly all tissues including striated muscle and the brain and this reduces its specificity as a biochemical marker for myocardial injury. • CK values are the first to rise after an AMI, and the first to return to normal if no further coronary damage occurs
CK-MB • CK-MB: An isoenzyme of CK which is more specific to myocardial tissue • Remains the most widely used enzyme marker, and is still the preferred marker for the diagnosis of AMI • More specific than CK for MI • The MB fraction is found predominantly in cardiac muscle. It is important to show both a rise in the serum concentration of CK-MB, and a rise in the ratio of CK-MB to total CK to diagnose MI
LDH • Lactate Dehydrogenase (LDH):Isozymes composed of combinations of two different subunits "H" and "M". • Subunit "H" predominates in heart muscle LDH which is geared for aerobic oxidation of pyruvate. • Rises acutely on initiation of an AMI. However, they take 2-3 days to reach maximum and thus do not play a major role in the diagnosis of AMI.
CK INDEX • CK-Index: The ratio of CK-MB to total CK • In AMI the value rises 5-15 folds and takes 24hrs to reach maximum. A low percentage can suggest the CK to be from a purely skeletal source and therefore rule out the possibility of MI.
CASE A: • Mr HA, aged 60 years, was brought in to A&E complaining of chest pain, nausea and a suspected AMI.
CK-MB Index • [CK-MB in ng/mL] / Total CK in U/L 100
Consistent with AMI? • The level of CK-MB in Mr HA’s clinical chemistry results follows the classic pattern of rise and fall related to a cardiac event. • The usual pattern of CK-MB levels after an AMI: • Increase 3-10hrs after the onset of infarction • Peak at 12-24hrs • Return to baseline after 36-72hrs
Consistent with AMI? • Mr HA’s clinical chemistry shows the CK-MB levels from the time of admission to A and E • Therefore, we can reasonably conclude that the results have shown that an AMI has occurred. • Based on this assumption, these results are consistent with an AMI
CURRENT CRITERIA • Mr HA, aged 60 years, was brought in to A&E complaining of chest pain, nausea and a suspected AMI. • Outline the current criteria for diagnosing acute myocardial infarction
WHO CRITERIA • A clinical history of ischaemic-type chest discomfort • Changes on serially obtained ECG • A rise and fall in serum cardiac markers
CASE A • Outline the current criteria for diagnosing acute myocardial infarction and the role played by the measurement of serum levels of the enzymes CK-MB1 and 2 in diagnosis of myocardial infarction. Define the difference in measuring CK-MB activity compared to CK-MB mass
An Ideal Marker • Present early and in high concentration in the myocardium • Absent from non-myocardial tissue and serum • Rapidly released into the blood at the time of the myocardial injury • Creatinine kinase (CK) isoforms, CK-MB1 and CK-MB2 has long been upheld as biochemical standards for diagnosing AMI
Cardiac Markers • Cardiac troponin I and CK-MB1&2 and their ratio are lab tests that have improved the diagnostic accuracy of MI • Other markers compared to CK-MB
Identifying Risk Factors In ACS • Troponin I&T: are both important establishing risk stratification of patients with acute coronary syndrome • Also CK-MB isoforms have a superior role
CASE A • Outline the current criteria for diagnosing acute myocardial infarction and the role played by the measurement of serum levels of the enzymes CK-MB1 and 2 in diagnosis of myocardial infarction. Define the difference in measuring CK-MB activity compared to CK-MB mass
CK-MB mass Vs CK-MB activity • CK-MB activity measurements only measure enzyme catalytic activity • CK-MB mass measurements only measure the amount of CK-MB released regardless of its activity • Compare and contrast both these terms
CK-MB activity Activity is detected using electrophoresis and immunoinhibition, it has limited reliability due to interferences CK-MB mass Not subject to interferences mentioned in immunoinhibition Measure of CK-MB mass by immunoassay involving monoclonal antibodies is much reliable, sensitive and specific under 1µg/L CK-MB mass Vs CK-MB activity
CK-MB activity increases in MI in a greater extent (>6%) than in skeletal muscle trauma (<3%) Specific for late diagnosis but not sensitive enough for early use ie relatively non-specific and requires longer time CK-MB mass is increased in both skeletal muscle trauma and myocardial infarction Specific diagnosis marker at 6 hours of onset CK-MB mass Vs CK-MB activity
Cardiac Troponins • Troponins are complex regulatory proteins that are tightly complexed to the contractile apparatus of muscle cells. Different Troponins isoforms appear in different muscle cells. • Troponin T (cardiac selective) • Troponin I (cardiac selective) • Troponin C (non-cardiac selective) • Circulating levels are normally low, but they rise rapidly after an AMI
Advantages of Cardiac Troponins as Biomarkers of MI Cardiac troponins cTnT and cTnI: • High Sensitivity • High Specificity • Remain elevated in serum for a number of days giving it a long diagnostic window • Reference interval effectively zero giving very little background noise
Disadvantages of Cardiac Troponins as Biomarkers of MI • cTnT and cTnI measured in different laboratories show different results • Non diagnostic marker due to cardiac trauma other than an MI. • Ischaemic heart disease can exist even in the absence of a raised cardiac troponin level. • Cannot be used as an early marker (appear 3-6 hrs after MI) • Prolonged troponin levels do allow detection of re-infarction
Monitoring Following Thrombolytic Therapy With Streptokinase. • Trials clearly show that hospital and 30-40 day mortality are statistically related to the level of reperfusion at 90 minutes following thrombolytic therapy. • Kinetics of myocardial protein appearance in circulation, namely CK-MB, myoglobin, cTnI and cTnT, following their release from the injured myocardium, depend on infarct perfusion and can be used to assess coronary reperfusion early after administration of thrombolytic therapy.
Reperfusion Monitoring: The Use of Myoglobin • Compared to total CK activity, cTnI and cTnT release, myoglobin can be used very early (within 90 minutes of thrombolytic therapy) to detect reperfusion. • A myoglobin to total CK activity ratio of >5.0 obtained from a single sample taken at the time of admission predicts spontaneous reperfusion 90 minutes following thrombolytic therapy. • A single myoglobin measurement at 90 min after the start of therapy combined with clinical variables improve prediction of reperfusion.
Reperfusion Monitoring: The Use of Cardiac Troponins • Guidelines to assess reperfusion: • An increase of cTnT levels to >0.5 µg/mL at 60 minutes following therapy. • A relative increase in cTnT levels at 90 minutes following therapy of >6.8. • A 90 minute concentration/baseline concentration following therapy of <6.0