Download
1 / 45
470 likes | 939 Views
Ischaemic Heart Disease. Role of Surgery in Ischaemic Heart Disease. Chronic angina unstable angina Complications of myocardial infarction mitral regurgitation due to papillary muscle dysfunction/rupture post-infarction VSD (ventricular septal rupture)

E N D
Role of Surgery in Ischaemic Heart Disease • Chronic angina • unstable angina • Complications of myocardial infarction • mitral regurgitation due to papillary muscle dysfunction/rupture • post-infarction VSD (ventricular septal rupture) • post-infarction ventricular aneurysm
IHDAssessment • Clinical Factors • Coronary Anatomy (Arteriography) • Ventricular Function
Clinical Factors • Significant disability from moderate to severe angina • Class III or IV symptoms • ‘symptoms on ordinary activity or at rest’ • Unresponsive to optimal medical care • control of: • blood pressure • arrhythmias • metabolic abnormalities • treatment of associated illnesses • anaemia • hyperthyroidism • ABSTINENCE FROM SMOKING • optimal drug therapy • nitrates • ß blockers • calcium channel antagonists • ACE inhibitors • K+ channel openers
Canadian Cardiovascular SocietyClassification of Angina CLASS ACTIVITY I 'Ordinary physical activity does not cause angina'; for example walking or climbing stairs, angina occurs with strenuous or rapid or prolonged exertion at work or recreation. II 'Slight limitation of ordinary activity'; for example, angina occurs walking or stair climbing after meals, in cold, in wind, under emotional stress or only during the few hours after awakening, walking more than two blocks on the level or climbing more than one flight of ordinary stairs at a normal pace and in normal conditions. III 'Marked limitation of ordinary activity'; for example, angina occurs walking one or two blocks on the level or climbing one flight of stairs in normal conditions and at a normal pace. IV 'Inability to carry on any physical activity without discomfort - angina syndrome may be present at rest' Source: Circulation, vol. 54, p. 522, 1976
Canadian Cardiovascular SocietyClassification of AnginaUnstable Angina CLASS ACTIVITY IV 'Inability to carry on any physical activity without discomfort - angina syndrome may be present at rest’ IVa Symptom deterioration now controlled on additional oral medical therapy. IVb Continued pain symptoms despite maximal oral medical therapy. IVc Continued pain symptoms despite iv therapy
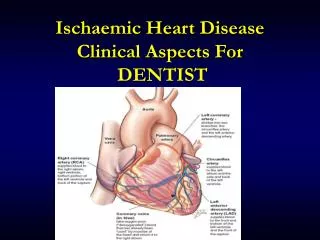
Coronary Anatomyarteriography • 75% luminal obstruction of a major branch • Adequate distal run-off • distal vessel free of lesions >25% • lumen diameter 1.5mm • 50% obstruction in LMCA
Ventricular Functiondirect relation to operative mortality • Ejection Fraction • Wall Motion Score • LVEDP
Anterobasal LA Anterolateral LV Apical Posterobasal Diaphragmatic Wall Motion Score • Normal • Moderate hypokinesia • Severe hypokinesia • Akinesia • Dyskinesia • Aneurysm
Case Study1 • 65yr male • angina x 7yr CCS III stable • dyspnoea on exertion NYHA III • MI x 2 1995, 2001 Risk Factors • Family history of IHD • Hypercholesterolaemia • hypertension • ex-smoker for 2months
Case Study 1 Medication Aspirin Clopidogrel Atenolol Diltiazem Ramipril Simvastatin Coronary Angiography Operation Coronary Artery Bypass Grafts without Cardiopulmonary Bypass 17/5/02 LIMA-LAD, LRA - OM1, PDRCA
Case Study 1 • Postop day 2 Atrial Fibrillation • commence on digoxin • rhythm return to sinus rhythm day 4 • Home on day 7 • Out-patient clinic review at 7 week postoperatively
Landmark Paper 1 • 10 year survival % • With LIMA 1VD - 93.4 2VD - 90.0 3VD - 82.6 • Veins only 1VD - 88 2VD - 79.5 3VD - 71.0 p=0.05 p=0.0001 p=0.0001 • x 1.6 risk of death • x 1.4 risk of late MI • x 2.0 risk of reoperation • Loop FD, Lytle B et al, N Engl J Med, 1986
Landmark Paper 2 • Two Internal Thoracic Artery grafts are better than one • Lytle B et al J Thorac Cardiovasc Surg 1999 • death, reoperation and PTCA were more frequent in single IMA group
Other Arterial Conduits? • right gastroepiploic artery • inferior epigastic artery • radial artery
Inferior Epigastric artery free graft
Coronary Artery Bypass Graftingoverall increased quality of life • Better relief of angina • Fewer limitations of activity • Reduced need for medication • Improved exercise tolerance testing
Coronary Artery Bypass Graftingoverall increased quality of life angina improved angina free
Perioperative Complications of CABG • Myocardial infarction 3-5% • Hypertension • Cathecolamines • Renin-angiotensin • Graft occlusion • Conduit damage during harvest • Inadequate distal run-off • Technical inadequacy
Case Study 2 • 54yr male • CABG x 3 ( LIMA - LAD, SVG - OM2, PDRCA) 1994 • Recurrence of angina 5yrs ago • CCS II Stable • Dyspnoea NYHA II Risk Factors • Hypercholesterolaemia • Family history of IHD • Ex-smoker 3months CVA 3yrs ago
Case Study 2 PMH • Cholecystectomy 6yr Drugs bisoprolol Atrovastatin Imdur Aspirin GTN Spray Coronary Angiography Operation 2/11/01 Redo CABG ( LRA - OM2 ) through L thoracotomy
Case Study 2 • Postop L Basal Atelectasis required physiotherapy • Home on day 6 • Reviewed at out-patient clinic at 6 weeks • Commenced cardiac rehabilitation programme
Return of Anginal Symptoms • Graft closure • Progress of lesions • New lesions
Case Study 3 • 71yr Male • CABG( SVG-LAD,OM1,RCA) 1985 • angina for 12 yrs CCS II Stable • dyspnoea NYHA IV • history of CCF Risk Factors • Hypercholesterolaemia • Hypertension • COAD • Ex-smoker
Case Study 3 Drugs Imdur frusemide Ramipril amlodipine Aspirin atrovastatin nicorandil LV angiography and coronary angiography Operation 14/1/02 LV Aneurysmectomy Postop- inotropic support for 3 days
Case Study 3 • Transferred to ward on day 5 • Home on day 10
Role of Surgery in Ischaemic Heart Disease • Chronic angina • unstable angina • Complications of myocardial infarction • mitral regurgitation due to papillary muscle dysfunction/rupture • post-infarction VSD (ventricular septal rupture) • post-infarction ventricular aneurysm
? Long Term Survival
Veterans Administration Co-operative Study (VACOOP) • European Coronary Artery Surgery Study (ECSS) • Coronary Artery Surgery Study (CASS) • Seattle Heart Watch (SHW)