Download
1 / 20
310 likes | 900 Views
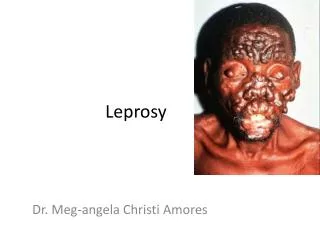
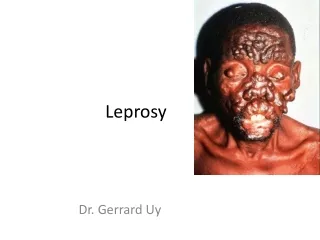
Leprosy. Leprosy (Hansen’s Disease). A chronic infectious disease caused by the bacterium Mycobacterium leprae It is mainly a Granulomatous disease affecting: peripheral nerves and mucosa of the upper-respiratory tract

E N D
Leprosy (Hansen’s Disease) • A chronic infectious disease caused by the bacterium Mycobacteriumleprae • It is mainly a Granulomatous disease affecting: peripheral nerves and mucosa of the upper-respiratory tract • Granulomatous - refers to granulomas which are lesions of epithelioid macrophages
A Little History … • Gerhard Henrik Armauer Hansen was a physician which first identified Mycobacterium leprae as the cause of leprosy in 1873 FYI 7/29/1841-2/12/1912
Pathology • Gram-positive • Intracellular • Aerobic rod-shaped bacillus • With a waxy coating • M. leprae is unable to grow in vitro • This is thought to be due to the fact that it no longer has the genes needed for independent growth • Because of its inability to grow on agar, nude mice and nine-banded armadillos are used as animal models
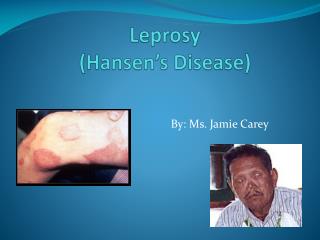
Clinical Features • Skin lesions, typically anaesthetic at the tuberculoid end of the spectrum • Thickened peripheral nerves • Acid-fast bacilli on skin smears or biopsy • Acid-fast is a property of Mycobacteria in which they a resistant to decolorization by acids during staining • This is a helpful diagnostic tool for M. tuberculosis and M. leprae
Symptoms Note: Contrary to popular belief leprosy does not cause bodyparts to simply fall off
Immunology • Tuberculoid leprosy • Patient’s lymphocytes respond to M. leprae in vitro • Skin tests with lepromin elicit a strong positive response • They also have a Th1- type response producing interleukin-2 and intergerons-γ • These strong cell-mediated responses clear antigens, but cause local tissue destruction • Lepromatous leprosy • Patients in this case do not mount a normal cell mediated response to M. leprae, and in fact their lymphocytes do not respond to M. leprae in vitro • They are also unresponsive to lepromin • They have specific T cell failure and macrophage dysfunction, and problems producing interleukin-2 and intergerons-γ • But they do produce Th2-type cytokins
Social Aspect • WHO reported that at the start of 2007 there were 224,717 reported cases (from 109 countries and territories) • In comparison with the number of new cases detected in 2006 which was 259,017, the number of new cases fell by more than 40,019 cases (a 13.4% decrease) • In the last five years, the global number of new cases has dropped on average by 20% per year. • Also Leprosy has been around since about 300BC FYI
Transmission • The transmission of leprosy is thought to occur through the respiratory track • Infected individuals discharge bacilli through their nose and a healthy individual breaths them in • But it is important to note that the extract mechanism is not known • The main reservoir is humans • Risk group: children, people living in endemic areas, in poor conditions, with insufficient diet, or have a disease that compromises their immunity (ie HIV) “In the 19th century leprosy was believed to be a hereditary ailment”
Diagnosis • Is clinical, by finding signs of leprosy and supported with the use of acid-fast bacilli smear or skin biopsy • But this is contingent on experienced histopathologist • What doctors typically look for include: anaesthesia of skin lesions, and peripheral nerve thickening and tenderness • There is no serological test Note: The genome has been sequenced
Treatment & Management • Chemotherapy • First line drugs are rifampicin, dapsone, and clofazimine • The WHO recommends that if a patient test positive in an acid-fast skin smear they should be treated for multibacillary disease • The patients bacterial load decides length of treatment (6-24 months) • Patients tend to improve quickly with minimal side-effects • Second line drugs are ofloxacin and minocycline • Triple –drug combinations have been used in cases where a patient has only a single lesion • Leprosy is combated with multidrug therapy to reduce the chance of developing resistance • Since in the 1960’s resistance to dapsone developed
Multibacillary (MB or lepromatous)is a 24-month treatment of rifampicin, clofazimine, and dapsone. Paucibacillary (PB or tuberculoid) is a six-month treatment of rifampicin and dapsone.
Treatment & Management • New Nerve Damage • Patients with motor or sensory loss of 6 moths or less should receive a 6 month treatment of corticosteroids (a treatment for type 1 reactions) • Patient Education • It is very important since within a few days of starting chemotherapy since patients will no longer be infectious and can live a normal life • Currently there are few leper colonies left • Also care of limbs is very important • Preventing Disability • Nerve damage produces anaesthesia, dryness and muscle weakness which in turn causes misuse of affected limbs causing ulceration and infection, leading to deformity • Dryness can lead to skin cracking and ultimately infection • Treatment involves soaking and applying oil- based creams to affected areas, also physiotherapy can help prevent contractures, muscle atrophy and over stretching of muscles
Treatment & Management • Immune-Mediated Reactions • Type 1 reactions occur in borderline leprosy • Type 1 reaction – delayed hypersensitivity occurring at site of localized M. leprae antigens • Skin lesions appear and are erythematous, and peripheral nerves become tender and painful • Loss of nerve function can be sudden (ie foot-drop) • Type 2 reactions occur in borderline lepromatous and lepromatous cases • Type 2 reaction – erythema nodosum leprosum (ENL) results from immune complex deposition • The main symptoms are malaise, fever, and crops of small, pink nodules on face and limbs, and ENL may continue for years • Management procedures include : control inflammation, pain, treat neuritis, and halt eye damage • Vaccines – there currently isn’t a vaccine against leprosy, but there are trials investigating the effectiveness of the BCG vaccine
Discussion Thalidomide (Thalomid). This drug was originally developed as a sedative and morning-sickness pill but was subsequently found to cause severe birth defects; the Food and Drug Administration then banned it. Under the new regulations there are a number of restrictions on its use: 1. It can be used only for the treatment of erythema nodosum leprosum. 2. Doctors who prescribe the drug and pharmacists who dispense it must register with Celgene, the company that produces it. 3. Women must have a negative pregnancy test 24 hours before taking the drug. 4. Women must get weekly pregnancy tests during the first month of treatment. Thereafter they must get once-a-month pregnancy tests. 5. All thalidomide users must enroll in a registry at Boston University that will record any pregnancies that occur and their outcomes. 6. All male patients must use condoms during sexual intercourse because the drug is found in semen. http://www.kcom.edu/faculty/chamberlain/Website/tritzid/leprosy.htm
Discussion 1) First of all let’s assume that areas with high concentrations of Leprosy could afford Thalidomide in addition to their basic treatment. What are the moral problems with its prescription? What are some of the additional problems that might arise if the above regulations aren't followed?
Discussion 2) What could explain such a drop in new Leprosy cases? Considering the expense and length of treatment, not knowing the mode of transitions and the fact that most areas that are affected are still developing. Free MDT, Reducing disease burden, Preventing disability, Changing the negative image, Working with local governments and agencies
I got this off the net, I hope it helps, if anyone has any questions please email me. Can leprosy cause limbs to fall off?Leprosy does not cause flesh to rot and fingers and toes to drop off. In the past, limbs that have been damaged because the person cannot feel pain have sometimes had to be amputated. Now that the disease can be detected early and cured completely, the need to amputate is very rare. Who can get leprosy? Susceptibility: About 90% of the population is not susceptible to infection. Children are more susceptible than adults. Immunologic and epidemiologic studies suggest that only 10-20% of those exposed to M. leprae will develop signs of indeterminate Hansen's disease; only 50% of those with indeterminate disease will develop full-blown clinical leprosy. Spontaneous healing also has been reported in tuberculoid leprosy. Host immunity: Where host cell-mediated immunity functions perfectly, organisms are routed and no disease develops. If the individual has good immunity, organisms are contained and TT disease occurs. In subjects with moderate immunity, a battle occurs and results in borderline types of leprosy. In persons with poor immunity, LL occurs.