Download
1 / 34
490 likes | 1.52k Views
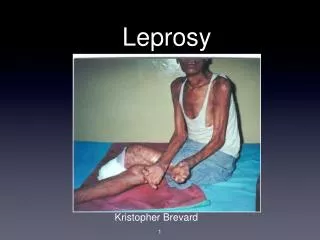
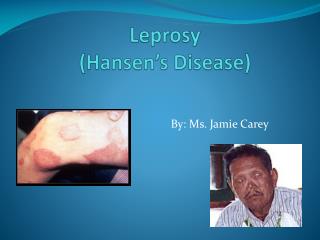
Leprosy Leprosy (Hansen ‘s disease ) is caused by the acid- fast bacillus Mycobacterium leprae.Unlike other mycobacteria , it does not grow in artificial media or even in tissue culture.Man is the only natural host of M. leprae.

E N D
Leprosy Leprosy (Hansen ‘s disease ) is caused by the acid- fast bacillus Mycobacterium leprae.Unlike other mycobacteria , it does not grow in artificial media or even in tissue culture.Man is the only natural host of M. leprae. The precise mode of transmission of leprosy is still uncertain but it is likely that nasal secretions play a role.Infection is related to poverty and overcrowding.Once an individual is has been infected ,subesquent progression to clinical disease appears to be dependent on several factors.Males appear to be more susceptible than females.
Two polar types of leprosy are recognized (Ridly-Jopling system): 1.Tuberculoid leprosy:a localized disease that occurs in individuals with a high degree of cell-mediated immunity(CMI).The T cell response to the antigen releases interferon which activates macrophages to destroy the bacilli (Th 1 response) but with associated destruction of the tissue.The lepromin test is positive. 2
2.Lepromateous leprosy: a generalized disease that occurs in individuals with impaired CMI.Here the tissue macrophages fail to be activated and the bacilli multiply intracellularly.Th 2 cytokines are produced. The lepromine test is negative. The WHO classification of leprosy depends on the number of skin lesions and the number of bacilli detected on the skin smears :paucibacillary leprosy has 5 or more fewer skin lesions with no bacilli ;multibacillary leprosy has 6 more lesions which may have bacilli. 3
Clinical features The incubation period varies from 2-6 years.The onset is generally insidious.Acute onset is known to occur , and the patients may present with a transient rash , with features of an acute febrile illness , with evidence of nerve involvement , or with any combination of these. 4
The major signs of leprosy are: 1.Skin lesions , usually anaesthetic ( generally tuberculoid ). 2.Thickened peripheral nerves , nerves of predilection which are superficial or lie in fibro-osseous tunnels- ulnar(elbow ), median (wrist ) ,radial cutenous(wrist ),common peroneal ( knee), posterior tibial and sural ( ankle) , facial (crossing zygomatic arch ), and greater auricular( posterior triangle of the neck ). 5
The spectrum of disease can be divided into five clinical groups: 1.Tuberculoid leprosy The infection is localized because the patient has unimpaired cell-mediated immunity.The characteristic , usually single , skin lesion is a hypopigmented , anaesthetic patch with thickened ,clearly demarcated edges, central healing , and atrophy.The face , gluteal region and extremities are most commonly affected.The nerve leading to the hypopigmented patch , and the regional nerve trunck , are often thickened and tender. 6
Unlike other parts of the body ,a tuberculoid patch on the face is not anaesthetic.Nerve involvement leads to marked muscle atrophy.Tuberculoid lesions are known to heal spontaneously.The prognosis is good. 7
2.Borderline tuberculoid (BT)leprosy This resembles TT but skin lesions are usually more numerous , smaller ,and may be present as small ‘satellite’ lesions around larger ones.Peripheral but not cutaneous nerves are thickened , leading to deformity of hands and feet. 8
3.Bordeline(BB) leprosy Skin lesions are numerous, varying in size and form( macules, papules , plaques ).The annular,rimmed lesion with punched-out , hypopigmented anaesthetic centre is characteristic .There is widespread nerve involvement and limb deformity. 9
4.Borderline lepromatous (BL) leprosy There are a large number of florid asymmetrical skin lesions of variable form , which are strongly positive for acid- fast bacilli.Skin between the lesions is normal and often negative for bacilli. 10
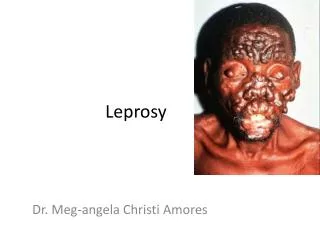
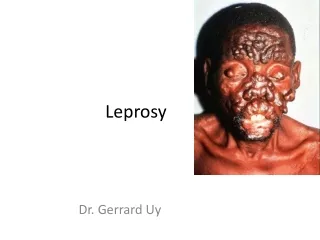
5.Lepromatous leprosy (LL) Although practically every organ can be involved , the changes in the skin are the earliestand most obvious manifestation.Peripheral oedema and rhinitis are the earliest symptoms.The skin lesions predominantly occur on the face ,the gluteal regions and the upper and the lower limbs.They may be macules , papules , nodules or plaques: of these , the macules is the first to appear.Infiltration is most noticeable in the ear lobes. 11
Thinning of the lateral margins of the eyebrows is characteristic.The mucous membranes are frequently involved , resulting in nasal stuffiness , laryngitis and horseness of voice.Nasal septal perforation with collapse of the nasal cartilages produces a saddle-nose deformity.With progression of the disease the typical leonine facies due to infiltration of the skin becomes apparent.Glove and stocking anaesthesia , gynaecomastia , testicular atrophy , ichthyosis and nerve palsies( facial , ulnar , median and radial) develop late in the disease.Neurotrophic atrophy affecting the phalanges leads to the gradual disappearance of fingers.Nerve involvement is less pronounced than in TT. 12
Lepra reactions These are immunologically mediated acute reactions that occur in patients with the borderline or lepromatous spectrum of disease , usually during treatment.Two forms are recognized : 13
A.Non-lepromatous lepra reaction ( type 1 lepra reaction ) This is seen following treatment of patient with borderline disease ; it is a type IV delayed hypersensitivity reaction.Both upgrading ( or reversal ) reactions ( i.e. a clinical change towards a more tuberculoid form) and downgrading reactions ( i.e. a change towards the lepromatous form ) can occur.Neurological deficits such as an ulnar nerve palsy may occur abruptly. 14
B.Erythema nodosum leprosum (ENL; type ll lepra reaction ) This is a humoral antibody response to an antigen-antibody complex ( i.e. a type lll hypersensitivity reaction).It is seen in 50% of patients with treated LL.ENL is characterized by fever , arthralgia , iridocyclitis , crops of painful , subcutaneous erythematous nodules, and other systemic manifestations.It may last from a few days to several weeks. 15
Diagnosis The diagnosis of leprosy is essentially clinical with: *Hypopigmented/ reddish patches with loss of sensation. *Thickening of peripheral nerves. *Acid –fast bacilli(AFB) seen on skin- slit smears/ biopsy.Small slits are made in pinched skin and the fluid obtained is smeared on a slide and stained for AFB. N.B…..patients should be examined carefully for skin lesions in adequate natural light.Occasionally nerve biopsies are helpful.Detection of M.leprae DNA is possible in all forms of leprosy using PCR. 16
Management Multidrug therapy (MDT) is essential because of developing drug resistance ( up to 40% of bacilli in some areas are resistance to dapsone).Much shorter courses of treatment are now used: the current WHO recommended drug regimens for leprosy are : Multibacillary leprosy (LL,BL,BB ) *Rifampicin 600mg once –monthly , supervised *Clofazimine 300 mg once – monthly, supervised *Clofazimine 50 mg daily ,self-administered *Dapsone 100 mg daily ,self-administered Treatment continued for 6 months 17
Paucibacillary leprosy (BT,TT) *Rifampicin 600 mg once-monthly ,supervised *Dapsone 100 mg daily , self- administered Treatment continued for 6 months Single lesion paucibacillary leprosy *Rifampicin 600 mg *Ofloxacin 400 mg as a single dose *Minocycline 100 mg 18
*Longer therapy may be required in severe cases.Follow up including skin smears is essential. *Patient education is essential.Patients should be taught self- care of their anaesthetic hands and feet to prevent ulcers. *Leprosy should be treated in specialist centres with adequate physiotherapy and occupational therapy support. 19
Treatment of lepra reaction This is urgent , as irreversible eye and nerve damage can occur.Antileprosy therapy must be continued.Type II lepra reactions (ENL) can be treated with analgesics , chloroquine , clofazimine, and antipyretics.Prednisolone 40-60 mg daily for 3-6 months is effective in type I reactions. 20