Download

1 / 29
310 likes | 467 Views
Testicular tumours. Urology 2012 . Case presentation. History 25 C/o hemoptysis, abdominal discomfort; History of UDT, right side-operated No child. 2. On exam: Generally well Scar R groin Nodes palpable, inguinal Big R testis, normal L testis What next?. Outcomes.

E N D
Testicular tumours Urology 2012
Case presentation • History • 25 • C/o hemoptysis, abdominal discomfort; • History of UDT, right side-operated • No child 2
On exam: • Generally well • Scar R groin • Nodes palpable, inguinal • Big R testis, normal L testis • What next?
Outcomes • Clinical presentation –age, Metastasis • Classification • Diagnosis • Differential diagnosis • Management
Epidemiology • Incidence • 2-3/100 000 in whites • <1/100 000 in blacks • R > L 2-3% bilateral • 95% Germ cell • Age • 16-35 yrs
Aetiology • Gonadal dysgenesis • Hereditary not clear • Environmental factors • Chemical carcinogens • Infections • 7-10% in undescended testis- Dysgenesis, temp, Abn blood supply, endocrine dysf(x)
Risk Factors • Previous history of testicular tumor • UDT • Infertility • Atrophic testis • CIS
Classification • Germ cell • Seminoma • Non seminoma • Embryonal • Choriocarcinoma • Teratocarcinoma • Yolk sac tumour • Mixed variant • Non Germ cell • Leydig cell • Sertoli cell • Sarcoma • leukaemia • Lymphoma • metastasis
Frequency • Seminoma -30% • Embryonal Carcinoma- 30% • Teratoma- 10% • Teratocarcinoma- 25% • Choriocarcinoma -1% • Combined- 15%o
Tumour markers • AFP • B-HCG • LDH
Metastatic pattern • Local • Lymphatic • hematogenous
Clinical presentetion • 50% have metastasis on diagnosis • 10% present with this as first sx • Neck mass, respiratory, GIT, bone pain, neurological, lower extremities • Local • Heavy feeling or painless swelling • 10% acute testicular pain • 5% Gynecomastia
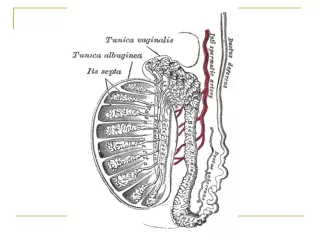
Examination • Local exam • Contra lateral vs. ipsilateral testis , • Epydidimis • Spermatic cord • Abdominal • General
Differential diagnosis • Testicular torsion • Epidydimo-orchitis • Hydrocoele • Inguinoscrotal hernia • paratesticular tumours
Investigations • Laboratory • Serum tumour markers • FBC, U&E,LFT`s • Radiological • Sonar • CXR • CT scan abdomen • Role of MRI?
staging • Clinical and surgical • Tumor type • degree of infiltration • Vascular invasion • Lymph metastasis • Distant metastasis • Serum tumor markers
Staging • A- confined to testis • B -Retroperitoneal spread • B1-3 • C- Metastatic disease • Or TNMS staging
Prognosis • Mortality • 50% in 1970 • Cure rate of > 95 % now! • Morbidity • Tumour related • Treatment related • Fertility?,QOL
Prognosis • Seminoma –overall cure rate is > 90% • Age – older patients • Sperm cryopreservation? • B HCG positive in 5-10% • very radio & chemosensitive
Non seminoma • Choriocarcinoma- Can present with extensive metastasiss with paradoxically small primary • Teratoma- mature and immature elements • Yolk sac tumour- In infants and young children
treatment • NB Multimodal • Radical orchidectomy • Radiotherapy • Chemotherapy • Retroperitoneal lymph node dissection • Follow up
General comments • Misdiagnosis common • No transscrotal biopsies • Good work-up • Quick referral • Follow up !
Other • Extragonadal germ cell tumours • Leydig cell – 10% malignant, present in children with virilising and in adults feminising. • Sertoli cell- any age.10% malignant • Gonadoblastoma- In dysgenetic gonads
Secondary tumours • Lymphoma • Leukaemic infiltration • Metastasis- prostate, Breast, kidney