Download
1 / 41
430 likes | 1.34k Views
Motor neuron disease. Multiple sclerosis. Motor neuron disease is degenerative disease which selectively affect motor tract fibers (corticospinal tract+ anterior horn cell) UMN signs LMN signs. Motor neuron disease. Motor pathway. cortex motor area

E N D
Motor neuron disease is degenerative disease which selectively affect motor tract fibers (corticospinal tract+ anterior horn cell) UMN signs LMN signs Motor neuron disease
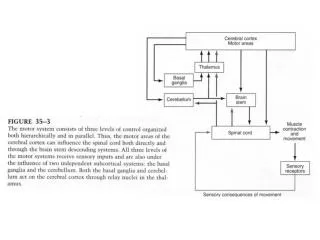
Motor pathway • cortex motor area • Corticospinal fiber & corticobulber • AHC motor neuron disease • Peripheral nerves • NMJ • muscle
pathology • Degeneration of the neurons
path physiology • Sporadic:90% unclear • Inherted:10% familial ALS,25% mutation in gene encoding copper zinc super oxide dismutase (SOD1)
course • Is progressive : median survival is approximately 3y
classification • Classic ALS (amyotrophic lateral sclerosis)..UMN+LMN signs • others • Progressive muscular atrophy • Primary lateral sclerosis • Progressive bulbar palsy • Progressive pseudo bulbar palsy
Classic ALS • Mixed upper motor neuron + upper motor neuron signs • Early patient may exhibit only LMN signs or upper LMN signs • Weakness begin a symmetrical and distally then spread to involve contiguous group of motor neurons • Bulbar &pesudobulber palsy involvement ..dysphagea & dysarthria
Nooooooooooo • Cognitive • Sensory • Ocular • Autonomic Sphincter dysfunction
diagnosis • El Escorial criteria for dx • Definitive • Probable • possible
Electrophysiological • NCS: sensory..N • motor:normal or dec amp • EMG: denervation
treatment • Riluzole :50 mg bid ( extend tracheotomy free survival by 2-3 months, not improving the survival or muscle strength • Supportive care physiotherapy, respiratory, swallowing…..
MS is the most disabling neurological condition of young adults
Epidemiology • Onset is typically in the mid 20s,although the dx may be delayed for several years • The ratio of f to m 1.77 to 1 • The incidence of MS in blacks residing in the united states is about 25% that of whites • High incidence includes all of Europe,North america,New Zealand,southern austeralia but the incidence also increasing in middle east
pathophysiogy • Inflamatory rxn causes variable tissue damage • Destruction of myelin producing cells (oligodendrocytes • Some cells damaged without remyelination but oligodendrocytes precursors ..remyelinate..plaque
Risk factors • Genetic • Infection :viral • autoimmune
genetic • In general in the united states, the prevalence of MS is about ,1% • If a mother has MS,, her children's have a chance 3-5% . • If father has MS, his son has a1% chance & his daughter a 2% chance • Non identical twins has 3-4% • Identical twins:30%
Clinical presentation • Relapsing remitting: the commonest • (>one attack in >one site (multifocal) • Progressive relapsing • Primary progressive • Secondary progressive
diagnosis • Clinical :typical relapses come on over a few days, lasts for weeks or months ,and then clear, over 80% of patients begin with relapses • All central nervous system can be affected • Typical relapses • A-optic neuritis • B-myelopathy(spinal cord) • C-brain stem &cerebellar
Optic neuritis: clouding or blurring of central vision in one eye • loss of measured activity, impair pupillary light reflex, some local pain made worse by eye movement…usually full recovery • Myelopathy: often sensory only; numbness &tingling from a certain level on the trunk on down through the rest of the body. if marked ..weakness • Brain stem
Each of these relapses may leave some residual • After several attacks of various types, a patient may present common deficit • Mild reduction in vision in one eye • No conjugate eye movements • Extensor planter responses &inability to walk heel and toe • Reduced vibration sense in the legs • Urgency of bladder function
Late stage deficit include: dementia, inability to stand or walk, slurred speech, ataxic, incontinence ,and marked sensory loss in hands &legs
Lehrmit sign • Athoufs phenomena
Diagnostic workup • MRI
Mri is now the dominant laboratory method of diagnosis in MS • MS lesions are usually easily detected and often characteristic… • Multiple bright lesion in T2 • Contrast enhanced lesion • Shape :ovoid • Size:>5mm • Site: adjacent to the lateral ventricles, corpus callosum, cerebellum
LP: modest no of lymphocytes <50/mm,total protein <.8g/L,elevated immunoglobulin G(IgG), level oligoclonal banding on electrophoresis(80%) • Evoked potentials: VER,BAR,somatosensory evoked potential
diagnosis • McDonald criteria: • Confirm lesion >one site +> one attack
Diffrential diagnosis • Clinically: • Multiple infarctions • Autoimmune diseases • Vascuilities: behcets • Sarcidosis • Infection: chronic meningitis
Diseases that cause similar MRI pictures • Vascular: vascuilities,small vesseles disease,migraine • Infection:HIV.Lyme disease • Granulomtous :sarcidosis • ADEM
Treatment: • Definitive supportive
definitive • Six principles of management in multiple sclerosis • 1-relapses with significant impairment of function should be treated with high dose IV corticosteroid • 2-All relapsing remitting patients should be receiving long term immunomodulatory treatments • 3-Secondary progressive need aggressive tt early,late tt <few years little benefit
4- primary progressive patients can not be expected to response to any tt • 5-multiple sclerosis is a life long disease ,no specific time when to discontinue tt once it started,if one modality of tt fail or not tolerated ,another medication shouled be tried • 6-patients need to be watched for signs of disease activity by clinical or magnetic resonance monitring or bothor both.
Drug used for long term management • Interferon –B(avonex,betaseron,rebif..dec the risk of the attacks by 30%(sc.IM) • Side effects: • Depression,flu like,hepatitis • Copaxon: • Widespread articaria
Drug for acute phase • Methylpredinsolone 1g iv for 5d • Side effects:
Supportive care symptomatic) • Spasticity • Depression • Fatigue • Urinary urgency • pain